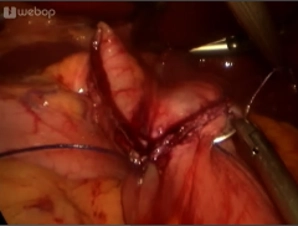
After starting the operation (Creating the pneumoperitoneum, working trocar placement, exploring the abdominal cavity) expose the angle of His.
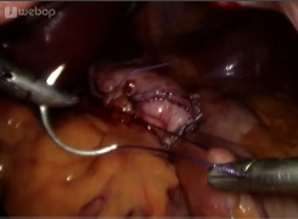
Then begin fashioning the gastric pouch at the lesser curvature 2 cm inferior to the gastroesophageal junction. In order to avoid bleeding complications and assure blood flow to the pouch, spare the left gastric artery which will supply the gastric pouch. Begin dividing the stomach in a horizontal direction with a linear stapler (staple height 3.5 mm).
Continue the dissection in triangular fashion toward the left crus of diaphragm. It serves as an anatomical landmark.
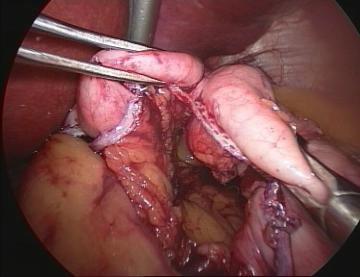
Transect the entire gastric fundus to bypass the production site of the enterohormone ghrelin from the intestinal transit and prevent subsequent dilation.
Finally, ensure adequate ultrasound hemostasis at the staple line.