
Median skin incision with left circumcision of the navel. Transection of subcutaneous fat tissue and fascia with diathermy.
-
Laparotomy
Soundsettings -
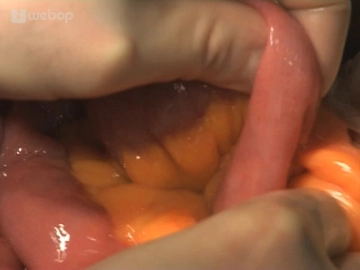
Exploration
![Exploration]()
Soundsettings Insertion of a drape and a retractor. Then determine the tumor size and location: The tumor is palpable just below the left flexure. Subsequently, review the abdomen to exclude metastases.
-
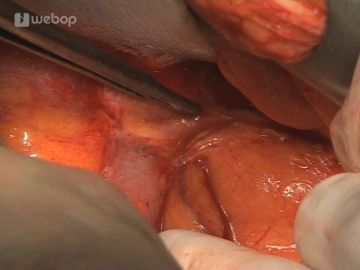
Determination of the oral resection margin
![Determination of the oral resection margin]()
Soundsettings The proximal resection margin depends on the location and size of the tumor. After identifying the middle colic artery, loop the transverse colon slightly distal to it. In the present case, the middle colic artery is not centrally resected due to the advanced age and the distant location of the tumor.
-
Mobilization of the descending colon and sigmoid colon
![Mobilization of the descending colon and sigmoid colon]()
Soundsettings The small intestine is held laterally to the right; the descending colon and sigmoid colon are released from the lateral adhesions. In doing so, at the level of the tumor, the plane of dissection must be led out of the peritoneal fold, as the tumor appears to be penetrating the serosa.

Entering the omental bursa
Opening of the omental bursa by detaching the greater omentum from the transverse colon to the left
Opening of the omental bursa by detaching the greater omentum from the transverse colon to the left
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.20
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.14 / module
US$85.75/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.29
/ month
US$171.50 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.