
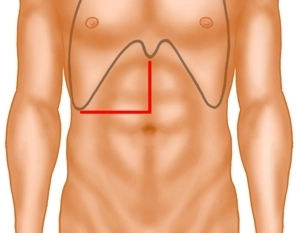
The laparotomy begins with a right-sided transverse incision at the level of the navel and is then extended in the midline supraumbilically to the xiphoid. Examination of the abdominal organs to exclude further metastases, confirmation of resectability.

Active local hemostasis and sealing
TachoSil® Versiegelungsmatrix
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for improving hemostasis, for supporting tissue sealing, and for suture support in vascular surgery when standard techniques are insufficient. TachoSil® is used in adults for supportive sealing of the dura mater to prevent postoperative cerebrospinal fluid leakage after neurosurgical procedures.
Produktwebsite TachoSil®
TachoSil® Prescribing Information 05-2025 (354.1 kB)