The surgical technique is demonstrated using a multinodular goiter II°. The procedure begins on the right side.
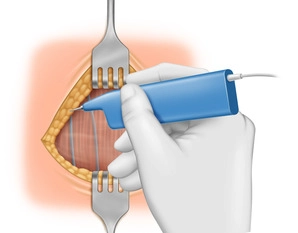
Cervicotomy (Kocher incision) in the area of the previously marked skin incision approximately 2 fingerbreadths above the jugulum.
Tip:
A skin incision placed too low can lead to keloid formation.
For large goiters, the incision should be placed higher, as it will lower after the goiter is removed.