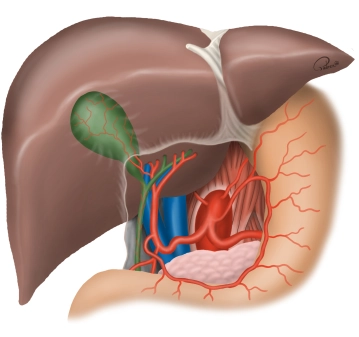
The bile duct transports bile from the liver to the duodenum. In this way, bile contributes to the digestion of fatty foods. The bile ducts begin intrahepatically with the right and left hepatic ducts (D. hepaticus dexter et sinister), which descend from the liver. When they converge, these two ducts form the common hepatic duct. As this duct continues to the duodenum, it joins with the cystic duct, which comes from the gallbladder (Vesica biliaris). Together, they form the common bile duct, which opens into the duodenum. The major duodenal papilla (Vater's papilla) acts as a sphincter that regulates the flow of bile from the common bile duct into the duodenum.
-
General Anatomy
![General Anatomy]()
-
Special Anatomy
The arterial supply of the gallbladder occurs in 75% of cases via a single cystic artery, which branches from the right hepatic artery running dorsally to the right hepatic duct (see figure above). In the remaining cases, the cystic artery branches from other branches of the hepatic arteries or from the gastroduodenal artery and runs ventrally to the common hepatic duct, or multiple arterial branches lead to the gallbladder. If there is an unclear bleeding during the operation, it usually stops by compressing the hepatic artery in the hepatoduodenal ligament or after placing a vascular clamp supraduodenally (so-called Pringle maneuver). Persistent bleeding may indicate an accessory hepatic artery from the superior mesenteric artery!
Anomalies of the cystic duct are less common than vascular variations but are of greater importance regarding the risk of injuries to the common bile duct. The cystic duct can enter the bile duct system at any point, including the papilla. Accordingly, the length of the cystic duct varies, it can be very short or absent, spiral in front of or behind the common hepatic duct, or share a common wall with it (duplication of the common bile duct). Additionally, accessory bile ducts from the liver can enter the cystic duct, the gallbladder, or the right hepatic duct. If the cystic duct is not clearly visible, there is the possibility of opening the gallbladder and probing the duct from the inside. Alternative: in unclear situations, intraoperative cholangiography!
Injuries to the common bile duct result from anatomical anomalies or disease-related changes. Excessive traction on the cystic duct can lead to placing the resection clamp too deeply, so that the edge of the choledochus is captured and ligated! This then leads to transection or stenosis of the main bile duct.
-
Functional liver anatomy
![Functional liver anatomy]()
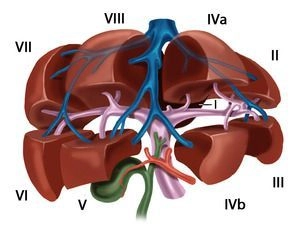
Through the falciform ligament and the insertion of the round ligament of the liver on the diaphragmatic as well as the sagittal fissure on the visceral surface, the liver is macroscopically divided into a larger right and a smaller left lobe (volume ratio approximately 80:20), although this morphological division does not correspond to the functional structure of the liver. The functional segmentation of the liver is determined by the branching of the portal structures: portal vein, hepatic artery, and bile duct. These three anatomical structures branch not only at the hepatic hilum but also predominantly in the same direction within the parenchyma. Each liver segment is completely independent in terms of blood supply and bile drainage from the other segments and can be surgically removed without endangering the function of the remaining liver.
The term "functional anatomy" thus refers to a sub-structuring of the liver, which is based on the delineation of hemodynamically independent parenchymal areas, and knowledge of which is essential for the surgical strategy in liver resection procedures.
-
Portal vein and hepatic veins
The functional division of the liver is based on the portal branching into individual, independent subunits, the segments.
Typically, the portal vein divides in the hepatic hilum into a right and left main branch. The boundary of these supply areas lies in the Cava-Gallbladder line ("Cantlie line"). By further bifurcation of each portal vein branch, an anteromedial and a posterolateral trunk for liver segments V/VIII and VI/VII are formed on the right side. The left main branch runs transversely to the left and then as the umbilical part anteriorly, ending at the insertion site of the Ligamentum teres hepatis in the so-called Recessus rex. The left portal main branch gives off branches for the two left-lateral segments II and III as well as for the median segments IVa and IVb. The caudate lobe holds a special position, as it can receive strong inflows from both the left and right portal main branches.
According to Couinaud, eight portal venous liver segments are distinguished, numbered clockwise starting with the caudate lobe as segment I:
Segment I
Caudate lobe
Segment I/II/III
Lateral left liver lobe
Segment IV
Left paramedian sector (Quadrate lobe)
Segment I/II/III/IV
Left liver half
Segment V/VIII
Right paramedian sector
Segment VI/VII
Right lateral sector
Segment V/VI/VII/VIII
Right liver half
The liver is traversed in a caudocranial direction by three main venous trunks, namely the right, middle, and left hepatic veins, which divide the liver into a total of four hepatic sectors. The left hepatic vein drains almost exclusively the left-lateral liver lobe and usually joins the middle hepatic vein shortly before its entry into the vena cava, which runs along the Cava-Gallbladder line. The right hepatic vein runs between the posterolateral and anteromedial segments. The caudate lobe has an independent venous outflow consisting of multiple small veins that drain directly into the vena cava dorsally, known as the Spieghel veins.
The portal hila of liver segments II, III, and IV are extrahepatic and can be relatively easily dissected in the anterior section of the left umbilical fissure. The hila of the right liver segments are intrahepatic. Exceptions occasionally occur, mostly involving segment VI. The anatomy of the hepatic veins is even more variable than that of the portal vein.
Variants
Portal vein system
- Anomalies of the portal vein bifurcation almost always affect the right portal main branch
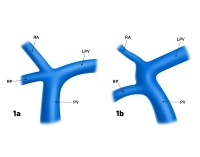
- Portal vein trifurcation: right main branch is absent, instead, there are two branches for the right double segments V/VIII and VI/VII (Fig. 1a); occasionally, one of the right branches may also originate from the left portal main branch (Fig. 1b)
- Variants of the left portal vein system rarely affect the main branch but almost always the division: several small portal vein branches instead of two segmental branches IVa/IVb, occasionally also an additional intermediate branch between the segmental branches II and III
![15_LAV_01_a_b_Pfortader_Lebervenen]()
Fig. 1a and 1b: PV = portal vein, LPV = left portal vein, RA = right anterior portal branch, RP = right posterior portal branch
Hepatic veins
- Variants of the hepatic veins are more common than those of the portal vein system
- Deviations from the hepatic sectors described by Couinaud particularly affect the territories of the right and middle hepatic veins
Hepatic arteries
The common hepatic artery originates from the celiac trunk, in rare cases, it originates directly f
The common hepatic artery originates from the celiac trunk, in rare cases, it originates directly f
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.20
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.14 / module
US$85.75/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.29
/ month
US$171.50 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.