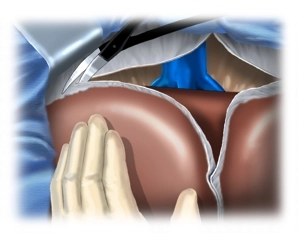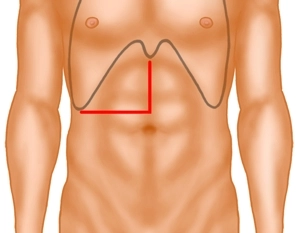
For the laparotomy the median incision is extended into the right flank just above the umbilicus Transect the right rectus muscle with bipolar scissors and incise the peritoneum. The incision may be kept to the left of the xyphoid: This yields good distance which facilitates the view, particularly regarding the hepatic veins.
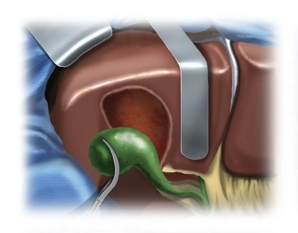
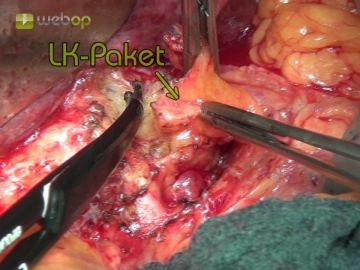
Now transect the falciform ligament close to the abdominal wall. After lining the wound edges with towels insert the retractor for the abdominal wall and inspect the field: In primary cancer of the liver rule out extrahepatic metastasis and noticeably large lymph node in the hilum; in the example demonstrated here there is cirrhosis of the liver
Note:
Smaller procedures on the left hepatic globe, up to and including left lateral resection, may also be performed via median laparotomy, and wedge excisions of the inferior segments IVb, V and VI via a subcostal incision.