
The existing skin scar is completely excised.
-
Excision of the skin scar
![Excision of the skin scar]()
Soundsettings -
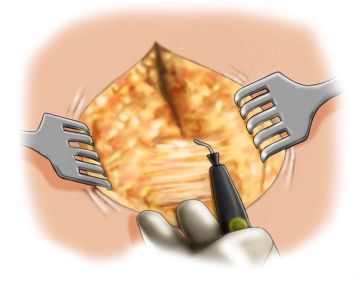
Exposure of the fascial defect
-
Opening of the abdominal cavity
-
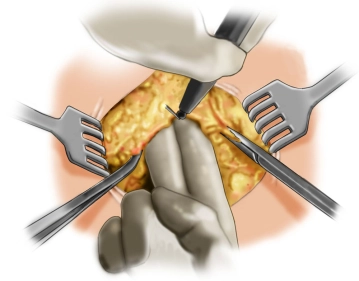
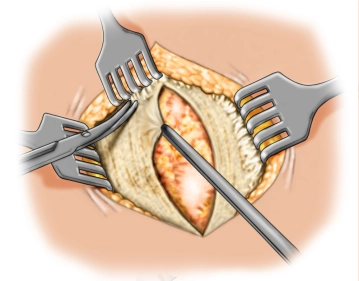
Local adhesiolysis
![Local adhesiolysis]()
Soundsettings The local adhesiolysis of visceral organs from the hernia sac and the adjacent abdominal wall allows for better visualization, preventing iatrogenic bowel lesions during further preparation of the omental bed. Subsequently, the abdominal cavity is protectively covered with a warm, moist cloth.
Note: An inter-enteric adhesiolysis should only be performed if there are corresponding symptomatic complaints.
-
Preparation of the anterior fascia
-
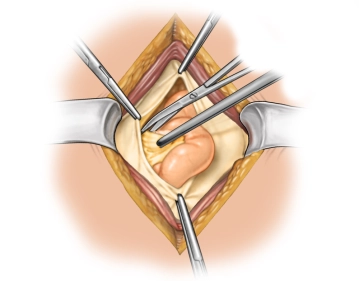
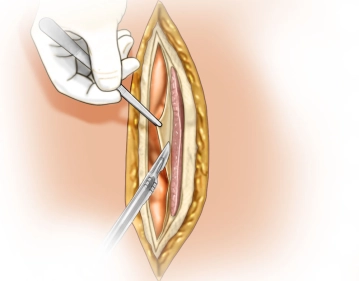
Incision of the rectus sheath
![Incision of the rectus sheath]()
Soundsettings Incision of the rectus sheath from the fascial edge on both sides of the linea alba with opening of the retromuscular space and mobilization up to the lateral edge of the rectus sheath. The opening of the rectus sheath should be as medial as possible to obtain sufficient anterior fascia for the planned fascial closure. During further lateral dissection, attention should be paid to the segmental vascular connections of the epigastric vessels and these should be preserved if possible. The goal is to prepare a sufficiently large mesh bed on both the left and right sides.
Preparation of the mesh bed
The goal is to prepare a sufficiently large mesh bed with a support of at least 5 cm not only later
The goal is to prepare a sufficiently large mesh bed with a support of at least 5 cm not only later
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.19 / module
US$86.33/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.38
/ month
US$172.70 / yearly payment