
Reinforcement of the posterior wall of the inguinal canal by laparoscopic insertion of a synthetic or biological mesh placed preperitoneally.
-
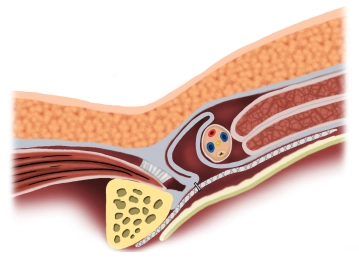
Principle
![Principle]()
-
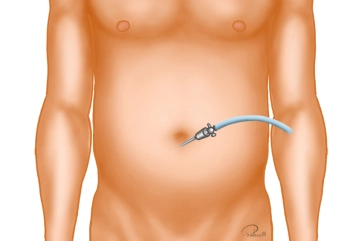
Creation of Pneumoperitoneum
![Creation of Pneumoperitoneum]()
Soundsettings A periumbilical skin incision approximately 1 cm long is made. Through this, the Veress needle is introduced, and the pneumoperitoneum is established. In cases of previous abdominal surgeries, the camera trocar is bluntly introduced via a mini-laparotomy.
Trocar positioning
The optical trocar (10 mm) is introduced bluntly with scissors after entering the abdomen and the a
The optical trocar (10 mm) is introduced bluntly with scissors after entering the abdomen and the a
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.23 / module
US$86.85/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.47
/ month
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.