
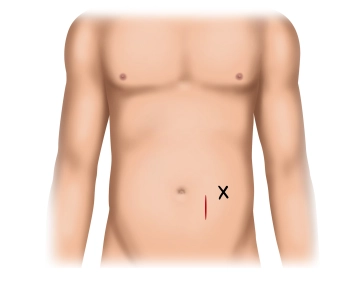
Approx. 6 cm long pararectal skin incision slightly caudal to the connecting line between umbilicus and skin marking for the catheter exit. Division of the subcutis using electrosurgical knife and exposure of the anterior rectus sheath.
-
Pararectal skin incision and exposure of the anterior rectus sheath
![Pararectal skin incision and exposure of the anterior rectus sheath]()
Soundsettings -
Exposure of the posterior rectus sheath layer and opening of the peritoneum
![Exposure of the posterior rectus sheath layer and opening of the peritoneum]()
Soundsettings Longitudinal incision of the anterior rectus sheath and blunt spreading of the rectus muscle. Opening of the peritoneum above the arcuate line and placement of the peritoneal suture at the caudal pole of the incision (PDS 3-0).
Tip:
- For stability reasons, it is recommended to perform the catheter implantation above the arcuate line.
- For the peritoneal suture, which also serves to anchor the catheter, a monofilament thread should be used to prevent tearing of the suture channels.
Placement of the Dialysis Catheter and Peritoneal Closure
Insertion of the CAPD catheter using forceps into the pouch of Douglas. In the subsequent cont
Insertion of the CAPD catheter using forceps into the pouch of Douglas. In the subsequent cont
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.