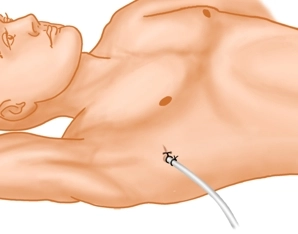
Note: For didactic reasons, the video was recorded in lateral position.
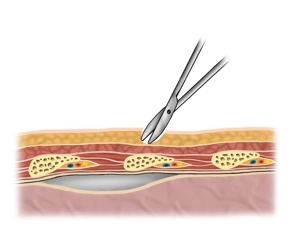
In the “Safe Triangle” between the lower edge of the pectoralis major muscle, the anterior edge of the latissimus dorsi muscle and the nipple line, a skin incision of 1-2cm is made directly at the level of the rib .
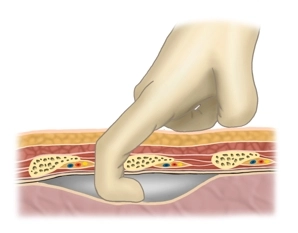
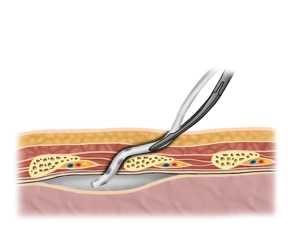
Tip: To avoid subcutaneous emphysema, the skin incision should be just wide enough so that the index finger can be easily passed through the incision. With the finger, blunt dissection can be performed and the drain placed under finger guidance.