The technique is demonstrated on a chronic recurrent pilonidal sinus.
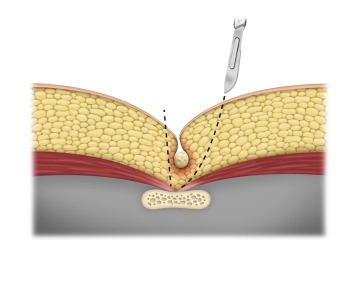
First, define the resection margins. The dotted lines correspond to the highest point of the buttock in question. The ovoid incision should be located eccentric to the midline and cover the entire system of tracts. The central axis of the incision should be about 2cm lateral to the midline.