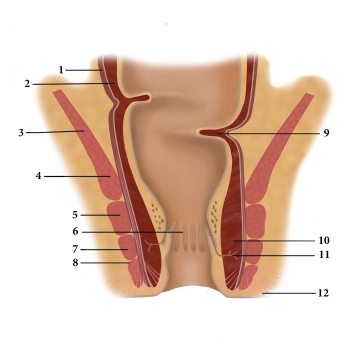
(1) Tunica muscularis, longitudinal sublayer, (2) Tunica muscularis, circular sublayer, (3) levator ani, (4) puborectalis, (5) external anal sphincter, deep part, (6) anal columns, (7) external anal sphincter, superficial part, (8) external anal sphincter, subcutaneous part, (9) Kohlrausch’s fold, (10) internal anal sphincter, (11) proctodeal gland, (12) corrugator cutis ani
Anal canal
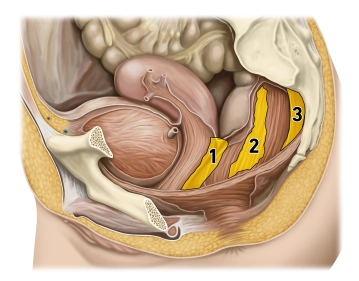
The interaction of three muscles in the lower rectum creates a sphincter mechanism:
1. The internal anal sphincter represents a thickening of the last annular fibers of the smooth colon muscles and is innervated by the sympathetic nervous system.
2. The levator ani, however, has voluntary innervation (sacral plexus) and includes the puborectalis arising from the symphysis pubis. Since the course of the puborectalis creates a sling (deficient anteriorly) around the rectum, the latter becomes angulated.
3. The external anal sphincter is also a striated muscle and extends from the center of the perineum (centrum perinei, perineal body) to the coccyx. Its somatic innervation is supplied by the pudendal nerve. With its contraction it completely seals off the anal canal.
The different innervation of the three muscles involved in the sphincter mechanism provides additional protection against failure and resulting incontinence.
The mucosa of the anal canal is plicated into numerous longitudinal folds (anal columns) displaying a dense arterial (!) plexus with venous drainage. When the sphincter muscles contract, these plexuses fill up quickly distending the mucosa and pushing the folds against each other, thereby ensuring a gas-tight seal. Hemorrhoids and venous thromboses are well known vascular complications in this region.
Defecation involves not only relaxation of the sphincter mechanisms (initiated by voluntary muscle action, drainage of the cavernous bodies) but also active abdominal press and intestinal peristalsis.