

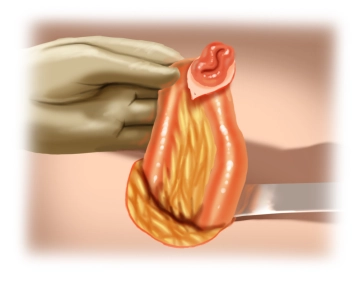
Oval excision of the stoma passage site with an approximately 2 mm wide skin margin and preparation through the subcutaneous tissue, possibly suturing the stoma (here fixation of the afferent loop with a holding suture for better mobilization and to prevent wound contamination with small bowel contents).
-
Skin Incision
![Skin Incision]()
Soundsettings -
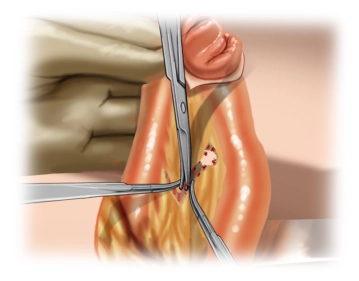
Mobilization and Preparation on the Fascia
![Mobilization and Preparation on the Fascia]()
Soundsettings Circular exposure of the afferent and efferent limbs near the intestine through the subcutaneous tissue down to the fascial level. Here, the stoma is released from the fascia on all sides with careful preservation of the small bowel mesentery. Preparation of the skin and subcutaneous tissue should only be as extensive as necessary for a secure intestinal suture. Excessive preparation increases the risk of hematoma and/or infection formation.
-
Mobilization of Small Intestine
![Mobilization of Small Intestine]()
Soundsettings After digital verification of complete release from the fascia, the stoma-bearing small intestine loop can be gently luxated in front of the abdominal wall.
-
Mesentery Preparation
![Mesentery Preparation]()
Soundsettings After mobilizing the small intestine, the skeletonization of the small intestine mesentery is performed immediately oral and aboral to the stoma opening only to the extent necessary to resect the stoma section.
Remarks:
Some surgeons prepare the scar edge remaining on the intestine to enable a direct anastomosis. For this purpose, the remaining skin portion is resected with scissors. It is important to ensure that the posterior wall of the intestine is preserved as broadly as possible. After checking the integrity of the mesentery, the continuous submucosal closure of the intestine is performed with a monofilament absorbable suture of size 4-0.
If the posterior wall bridge is too narrow, there is a circulatory disorder due to a vascular injury of the mesentery, or the intestinal segment to be anastomosed shows ischemia, a short-segment resection of the intestinal section with consecutive anastomosis is mandatory.
Since there are regularly problems with a too narrow posterior wall bridge, the short-segment resection with anastomosis should be regarded as a standard procedure. This can be performed end-to-end or, as in the present article, also side-to-side.

Resection Stoma
Resection of the stoma-bearing ileum segment (length: approximately 10 cm). This can be done sharpl
Resection of the stoma-bearing ileum segment (length: approximately 10 cm). This can be done sharpl
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.23 / module
US$86.85/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.47
/ month
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.