
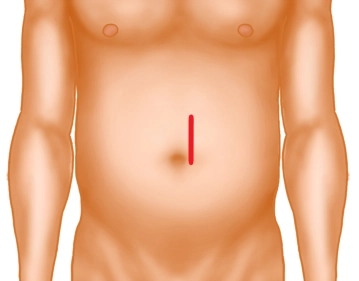
Small median laparotomy, depending on the location of the findings in the small intestine above the umbilicus, periumbilical or below the umbilicus.
It should be noted that laparotomies in the lower abdomen leave a cosmetically better result. The skin incision should be started with a length of about 8 cm. Through this, the small intestine can usually be adequately exteriorized and, if necessary, the skin incision can then be extended. As a rule, a left-sided circumincision of the umbilicus, if required, is common.
-
Skin incision
![Skin incision]()
Soundsettings -
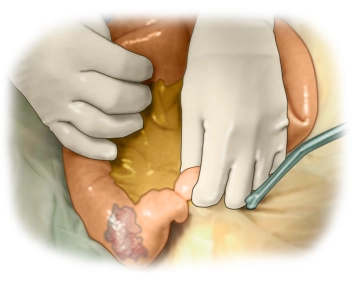
Retraction of the skin edges
![Retraction of the skin edges]()
Soundsettings When an anastomosis is performed, it is advisable to protect the skin edges by folding them over with a foil or a moist abdominal cloth and then to insert a retractor.
-
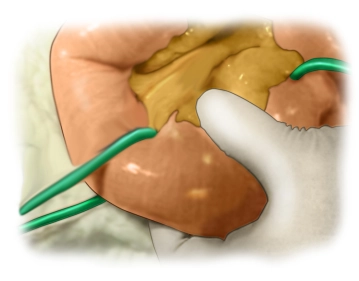
Eventration of the Small Intestine
![Eventration of the Small Intestine]()
Soundsettings The small intestine is eventrated and the finding is located. Whenever possible, the entire small intestine should be inspected, which, provided no adhesions are present, is usually possible through a correspondingly small surgical access.
-
Defining the Resection Boundaries
![Defining the Resection Boundaries]()
Soundsettings Subsequently, the resection boundaries are defined, e.g., by encircling with a rubber loop, which significantly facilitates visibility.
-
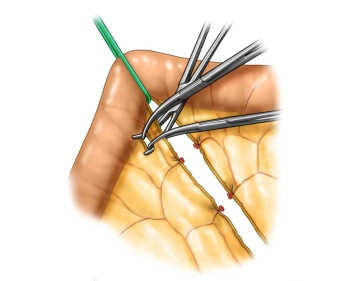
Transection of the Mesentery
![Transection of the Mesentery]()
Soundsettings Subsequently, the mesentery is gradually transected over Overholt clamps. Distally, towards the specimen, ligatures are applied. Centrally, the mesentery is secured with ligatures or sutures. Centrally, care must be taken to ensure that secure hemostasis is achieved here, so in case of doubt, it is better to use one more suture than one too few.

Preparation of the Side-to-Side Anastomosis
Especially if there is a lumen difference, as in the present case, it is advisable to perform a sid
Especially if there is a lumen difference, as in the present case, it is advisable to perform a sid
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.26 / module
US$87.13/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.52
/ month
US$174.30 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.