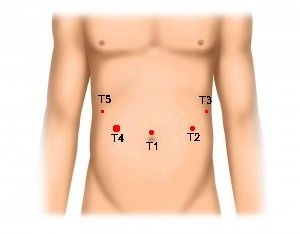
The procedure begins with marking the trocar positions on the abdominal wall. After inserting the Veress needle and pressure-controlled CO2 insufflation, the following trocars are placed in a semicircular arrangement:
- T1 = 10 mm optic trocar
- T2 = 10 mm working trocar
- T3 = 5 mm working trocar (later 12 mm for CEEA stapler and extension incision for specimen retrieval)
- T4 = 12 mm working trocar
- T5 = 5 mm working trocar