
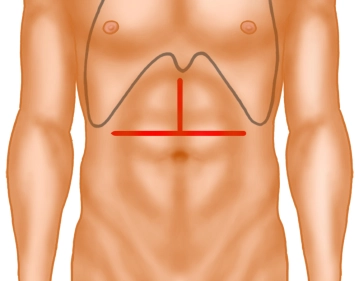
The opening of the abdomen is performed via a transverse upper abdominal laparotomy with upper median laparotomy, so-called “inverted T“.
Then, using diathermy, the subcutaneous tissue and subsequently the rectus musculature are transected along the linea alba.
The opened abdominal cavity is now explored to assess the location and extent of the tumor and thus the resectability after exclusion of distant metastases, especially on the peritoneum and liver. The tumor is located in the middle third of the stomach at the greater curvature.
-
Transverse Upper Abdominal Laparotomy
![Transverse Upper Abdominal Laparotomy]()
Soundsettings -
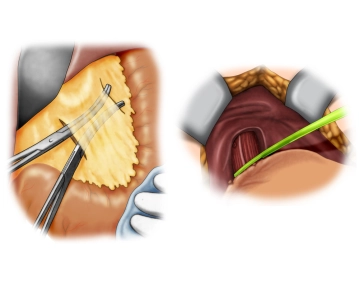
Detachment of the lesser omentum; Preparation of the gastroesophageal junction
![Detachment of the lesser omentum; Preparation of the gastroesophageal junction]()
Soundsettings After releasing pericholecystic adhesions, the lesser omentum is detached close to the liver from distal to proximal while sparing the hepatoduodenal ligament. The preparation then continues to the gastroesophageal junction. The abdominal esophagus is circumferentially exposed and looped.
-
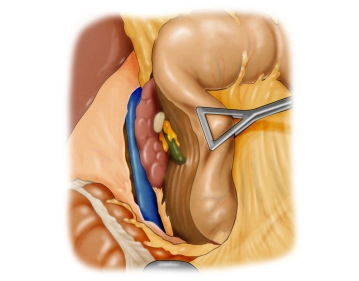
Kocher Mobilization
![Kocher Mobilization]()
Soundsettings Now follows the mobilization of the duodenum according to Kocher. In this process, the paraduodenal peritoneum is incised approximately 1 cm away from the lateral margin and the duodenum is elevated dorsally in a largely avascular plane from the retroperitoneum and the vena cava is exposed.
-
Preparation at the hepatoduodenal ligament
Soundsettings Start of the lymph node dissection at the hepatoduodenal ligament (LN group 12), during which the right gastric artery is transected close to its origin and the common hepatic artery is looped.
Detachment of the greater omentum and the gastroepiploic vessels
By dissecting the greater omentum from the transverse colon, the omental bursa is completely opened
By dissecting the greater omentum from the transverse colon, the omental bursa is completely opened
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.
TachoSil<sup>®</sup> Versiegelungsmatrix
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.