Median skin incision with left circumcision of the navel. Transection of subcutaneous fat tissue and fascia with diathermy.
-
Laparotomy
Soundsettings -
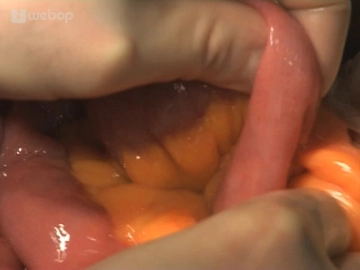
Exploration
![Exploration]()
Soundsettings Insertion of a drape and a retractor. Then determine the tumor size and location: The tumor is palpable just below the left flexure. Subsequently, review the abdomen to exclude metastases.
-
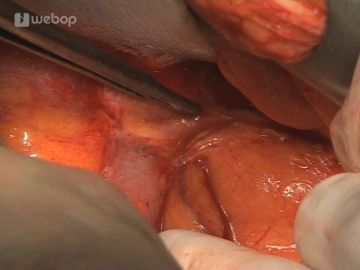
Determination of the oral resection margin
![Determination of the oral resection margin]()
Soundsettings The proximal resection margin depends on the location and size of the tumor. After identifying the middle colic artery, loop the transverse colon slightly distal to it. In the present case, the middle colic artery is not centrally resected due to the advanced age and the distant location of the tumor.
-
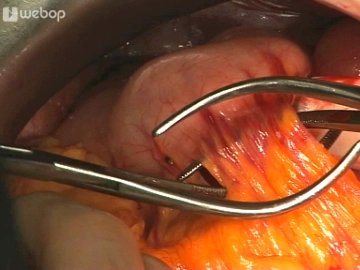
Mobilization of the descending colon and sigmoid colon
![Mobilization of the descending colon and sigmoid colon]()
Soundsettings The small intestine is held laterally to the right; the descending colon and sigmoid colon are released from the lateral adhesions. In doing so, at the level of the tumor, the plane of dissection must be led out of the peritoneal fold, as the tumor appears to be penetrating the serosa.
-
Entering the omental bursa
Soundsettings Opening of the omental bursa by detaching the greater omentum from the transverse colon to the left of the planned resection site. Transection of the splenocolic ligament with clamps for mobilization of the left flexure.
-
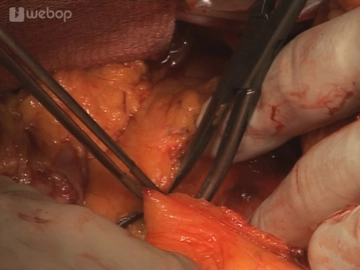
Detachment of the greater omentum from the stomach
![Detachment of the greater omentum from the stomach]()
Soundsettings Detachment of the greater omentum from the stomach including the gastroepiploic arcade.
Note: Including the gastroepiploic arcade in left hemicolectomy is not strictly necessary, but is done here for radicality reasons.
-
Transection of the greater omentum
Soundsettings Divide the greater omentum from its free edge towards the oral resection margin between Overholt clamps.
-
Mobilization of the left flexure
![Mobilization of the left flexure]()
Soundsettings After the connections to the spleen have already been severed, the suspension of the colonic flexure can usually be transected without further ligatures. Continuing this incision medially leads to the lower edge of the pancreas.
-
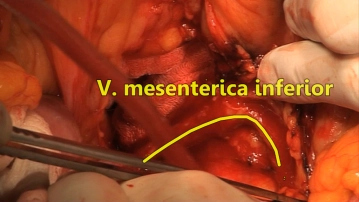
Transection of the left colic vein
![Transection of the left colic vein 1]()
![Transection of the left colic vein 2]()
Soundsettings Identification of the main vessels. Since no central ligation of the inferior mesenteric artery and vein is planned to preserve the distal sigmoid colon, dissection of the duodenum from the mesocolon with visualization of the inferior mesenteric vein. Subsequently, the origin of the left colic vein is exposed and transected.
-
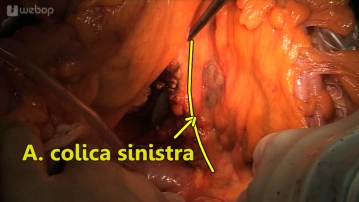
Dissection of the left colic artery
![Dissection of the left colic artery]()
Soundsettings Exposure of the left colic artery. Establishing the distal resection margin in the mid-sigmoid colon. Gradual transection of the mesentery with maximal inclusion of the lymphatic drainage area. The lymph nodes are initially dissected up to the trunk of the left colic artery and included. Resection of the left colic artery while preserving the superior rectal artery.
-
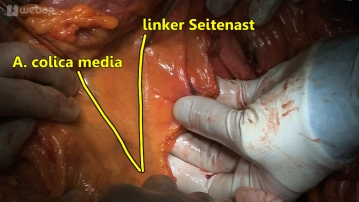
Transection of the mesocolon
![Transection of the mesocolon]()
Soundsettings Starting from the central detachment point of the vessels, the mesocolon is first transected towards the distal resection plane. Subsequently, incision of the transverse mesocolon begins centrally, involving the transection of the left branch of the middle colic artery and the marginal arcade.
-
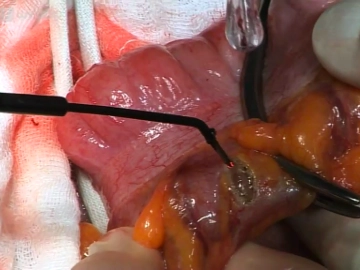
Transection of the intestine
![Transection of the intestine]()
Soundsettings Open transection of the colon at the defined resection margins with diathermy. Submission of the specimen.
-
Anastomosis of the colon
Soundsettings First, slit the end of the sigmoid colon to create congruent intestinal lumens. Then, perform a transverse sigmoidostomy in a single-layer continuous suture technique using a slowly absorbable monofilament suture of size 3-0 as an end-to-end anastomosis. Closure of the mesenteric slit is optional.
-
Drainage and wound closure
Soundsettings Rinsing of the abdomen and placement of a drainage in the left subphrenic area. Continuous fascial closure and subcutaneous suture, staple closure of the skin.