Reinforcement of the posterior wall of the inguinal canal by laparoscopic insertion of a synthetic or biological mesh placed preperitoneally.
-
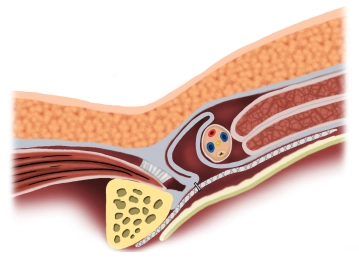
Principle
![Principle]()
-
Creation of Pneumoperitoneum
![Creation of Pneumoperitoneum]()
Soundsettings A periumbilical skin incision approximately 1 cm long is made. Through this, the Veress needle is introduced, and the pneumoperitoneum is established. In cases of previous abdominal surgeries, the camera trocar is bluntly introduced via a mini-laparotomy.
-
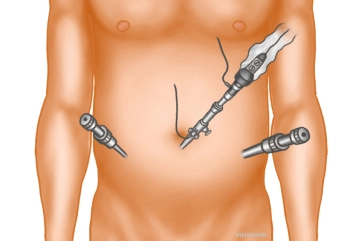
Trocar positioning
![Trocar positioning]()
Soundsettings The optical trocar (10 mm) is introduced bluntly with scissors after entering the abdomen and the abdominal cavity is inspected. Then, under direct vision, additional trocars are inserted laterally on both sides approximately at the level of the navel: a 5 or 10 mm trocar on the hernia side, and a 5 mm trocar on the opposite side.
Tip: The camera is guided so that the 30° optics face ventrally. This is the only way to obtain an overview of the posterior inguinal region.
Remark 1: If no inguinal hernia is visible upon inspection of the inguinal region, preparation should still be carried out, as the symptoms could be caused by the prolapse of a spermatic cord lipoma.
Remark 2: After placing the trocars, the operating table is positioned in the Trendelenburg position so that the intestines can be shifted to the upper abdomen and tilted 20° towards the surgeon to allow for better ergonomic working conditions.
-
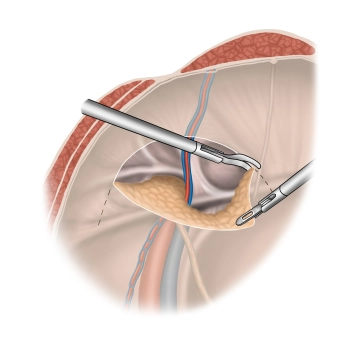
Peritoneal incision and preparation, presentation of the anatomical "landmarks"
![Peritoneal incision and preparation, presentation of the anatomical "landmarks"]()
Soundsettings The incision of the peritoneum begins after palpation from the outside in the area of the anterior superior iliac spine, runs in an arc 3-4 cm above the internal inguinal ring over the epigastric vessels, and ends at the medial umbilical fold. The fold itself should not be transected.
Note: Asymptomatic adhesions in the lower abdomen do not need to be resolved, as the actual hernia procedure is performed preperitoneally.
Medial to the epigastric vessels, dissection is performed between the bladder (beware of bladder injury) and the posterior rectus sheath to expose the dorsal side of the symphysis and the Cooper's ligament. Then, the peritoneum is bluntly dissected caudally from the epigastric vessels, the vas deferens, and the spermatic cord vessels.
-
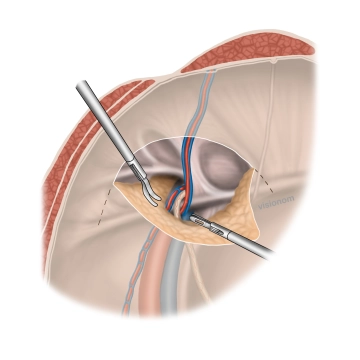
Exposure and repositioning of the hernia sac, mesh bed preparation
![Exposure and repositioning of the hernia sac, mesh bed preparation]()
Soundsettings Detachment of the hernia sac and peritoneum from the spermatic cord structures and the transversalis fascia or fascia iliaca to create a sufficiently large mesh bed. The ductus deferens and testicular vessels (vasa spermatica) are carefully lysed. Laterally, preparation is done up to about 4-5 cm below the iliopubic tract and medially up to about 2-3 cm below the pubic bone. No tissue strands should remain that could roll up the mesh during peritoneal closure and thus lead to a recurrence.
-
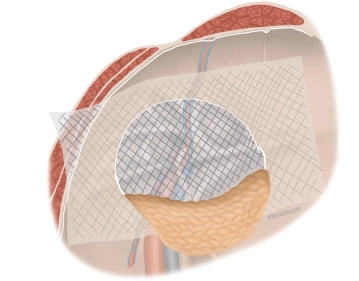
Insertion of the mesh
![Insertion of the mesh]()
Soundsettings A 12 x 16 cm bio-mesh is trimmed and marked. It is then rolled up and introduced through the periumbilical trocar access using a grasping forceps. Using grasping forceps, the mesh is positioned to cover all hernia openings.
For bilateral hernias, a second mesh is introduced and positioned in the same manner. -
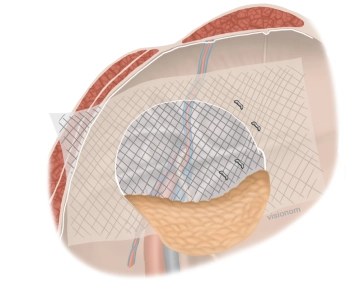
Mesh fixation
![Mesh fixation]()
Soundsettings In the example, it is a bio-network that requires a fibrin glue for fixation. The mesh is spot-fixed with the fibrin glue high medially on the ventral abdominal wall and caudally on Cooper's ligament.
Note 1: For synthetic meshes, a synthetic tissue adhesive can be used.
Note 2: When using staples, the possible course of the nerves must be considered. In the "triangle of pain" (bounded by the inguinal ligament, the testicular vessels or iliac vessels, and the peritoneal fold), the genitofemoral and lateral femoral cutaneous nerves should be considered. At the Cooper's ligament, the staple fixation must be performed strictly under visual control to avoid vascular injury (Corona mortis). When using tissue adhesives, the possible course of the aforementioned nerves must also be considered depending on tissue toxicity.
-
Closure of the peritoneal incision
![Closure of the peritoneal incision]()
Soundsettings The pneumoperitoneum is reduced to a pressure between 6-8mmHg and the peritoneal incision is closed with a continuous V-Loc suture 3-0. Then, placement of a Redon drain through the ipsilateral trocar access via a small peritoneal incision into the omental bed with subsequent suturing at skin level.
Not shown: Finally, the trocars are removed under direct vision and the pneumoperitoneum is released. Each access > 5mm is securely closed from the outside with fascial sutures, if necessary, with percutaneously placed fascial threads (thread catcher).