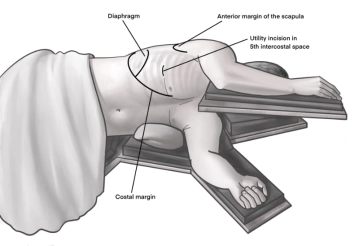
Incision of approximately 4 cm in length in the area of the anterior axillary line at the upper edge of the 5th rib to access the 4th intercostal space above. A helpful orientation is often an imaginary line from the tip of the scapula to the nipple. Transection of the subcutaneous tissue on the rib with the monopolar knife. Subsequently, stepwise preparation of the intercostal muscles with the monopolar knife. The pleura is opened bluntly with a finger. Palpation of the thoracic wall for adhesions and insertion of a wound protection film.
-
Access for uniportal VATS right
![Access for uniportal VATS right]()
-
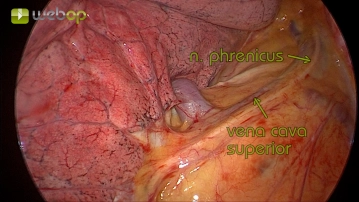
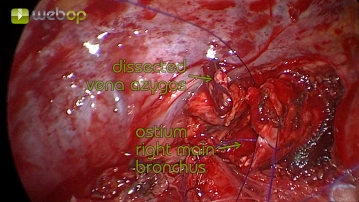
Preparation and dissection of the azygos vein
![Preparation and dissection of the azygos vein]()
Soundsettings First, the lung is luxated dorsolaterally, providing a view of the azygos vein. This is then freed from the pleural covering using an electric hook, bluntly dissected circularly, secured with titanium clips, and sharply transected.
Note:
- The resection of the azygos vein can be performed using clips, hand sutures, or a stapling device. Its transection facilitates the subsequent dissection and closure of the right main bronchus, although it is not mandatory.
-
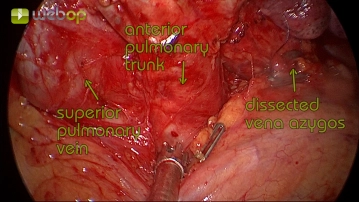
Preparation of the lung hilum and the pulmonary artery
![Preparation of the lung hilum and the pulmonary artery]()
Soundsettings After opening the mediastinal pleura, an incision with an electrocautery hook and blunt dissection of the mediastinal adipose tissue exposes the view of the lung hilum. Here, the anterior trunk of the central pulmonary artery is directly visible and is circumferentially dissected. The upper pulmonary vein is also clearly recognizable.
-
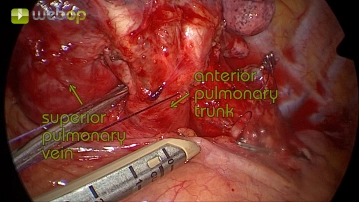
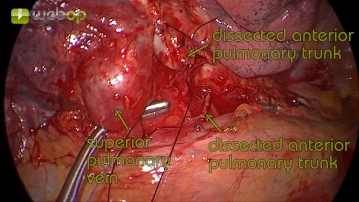
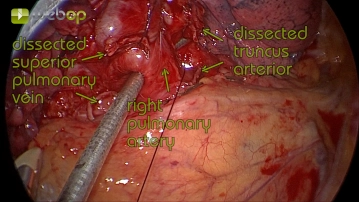
Dissection of the anterior trunk of the pulmonary artery
![Dissection of the anterior trunk of the pulmonary artery]()
Soundsettings After circular presentation and blunt dissection of the anterior trunk, it can be safely transected using an endoscopic stapling device.
Note:
- The separate resection of the anterior trunk is often not possible with more central tumors, but as in this case, it facilitates the resection of the central pulmonary artery.
-
Preparation of the upper pulmonary vein
![Preparation of the upper pulmonary vein]()
Soundsettings The superior pulmonary vein is already visible in the situs without further dissection. Typically, the middle lobe vein drains into the superior pulmonary vein and can be clearly identified there.
Note:
- Here, before transection of the superior pulmonary vein, the central pulmonary artery was looped with absorbable suture to avoid injury during resection of the superior pulmonary vein.
- The confluence of the middle lobe vein is not depicted here. Its depiction is not strictly necessary, but during further dissection, attention should be paid to whether it might still be in situ and either drains more centrally into the superior pulmonary vein or into the inferior pulmonary vein.
-
Resection of the central pulmonary artery
![Resection of the central pulmonary artery]()
Soundsettings After transecting the superior pulmonary vein, the view of the central pulmonary artery is unobstructed. The anterior trunk was already divided in step 4, allowing the entire remaining right pulmonary artery to be prepared here.
-
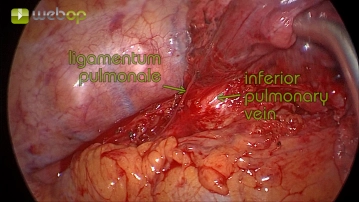
Preparation of the pulmonary ligament and the inferior pulmonary vein
![Preparation of the pulmonary ligament and the inferior pulmonary vein]()
Soundsettings Now the preparation in the pulmonary ligament is performed by stretching the lung apically until the lower pulmonary vein is exposed. This can now be bluntly dissected in a circular manner in the known way and then transected using a stapling device after traction.
-
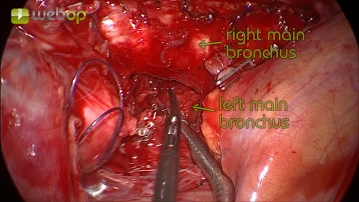
Preparation of the right main bronchus
![Preparation of the right main bronchus]()
Soundsettings By gently pulling the lung caudally, the right main bronchus can now be expanded. After circular, blunt dissection, resection can be performed using a stapling device or sharp transection and hand suture.
Note:
- To avoid circulatory disturbances and thus wound healing disorders with severe bronchial stump insufficiency, it is particularly important to use electricity sparingly here.
- To prevent complications, it is important that the bronchial stump is kept as short as possible.
-
Retrieval of the specimen
![Retrieval of the specimen]()
Soundsettings The entire right lung can be removed using an extraction bag through the 3-4 cm incision.
Note:
- Instillagel or similar lubricants can often be very helpful here.
- The use of an extraction bag is mandatory to prevent cell seeding or tearing of the lung parenchyma.
-
Suture of the bronchial stump
![Suture of the bronchial stump]()
Soundsettings This section demonstrates the endoscopic suture of the bronchial stump using a continuous double-layer technique with PDS 3-0 thread. Alternatively, a stapling device can be used. A short bronchial stump and an atraumatic technique when manipulating the bronchial edges are essential to avoid healing complications. Finally, after treating the bronchus, a leak test with water should always be performed.
-
Coverage of the bronchial stump
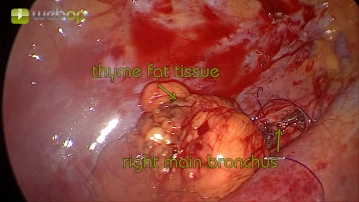
![Coverage of the bronchial stump]()
Soundsettings To prevent the serious complication of bronchial stump insufficiency, reconstruction and coverage with vital tissue can be performed. Here, thymic fat tissue is prepared from the pericardium until it lies tension-free on the bronchial stump and is then fixed with sutures. The goal is to ensure that the bronchial stump does not protrude uncovered into the pleural cavity.
Note:
- In right-sided pneumonectomies, covering the bronchial stump is advisable, as the necessary coverage is not provided by mediastinal structures as it is on the left side.
- The performance of plastic bronchial stump coverage can be done routinely, but should especially be considered in the presence of risk factors such as metabolic diseases, pre-existing cachexia or protein deficiency, or when adjuvant radio- and/or chemotherapy is required.
- In addition to the thymic tissue shown here, a pedicled pericardial fat flap can also be used for covering the bronchial stump.
-
Wound closure
Removal of the wound retractor and under direct vision, insertion of a 24 Charrière chest drain at the medial edge of the incision with ventrocranial orientation. After final hemostasis and checking the lung for tightness and ability to expand, the wound is closed. Removal of the wound protection film. Continuous suture of the serratus anterior muscle and the subcutis. Intracutaneous continuous skin suture.