
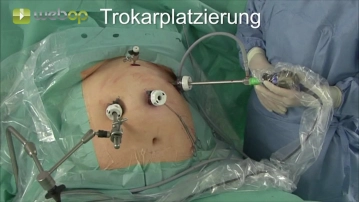
Position the camera trocar in the left upper quadrant, ensuring it is at least 15 cm away from the xiphoid.
Insert another two 12 mm trocars in the median epigastrium inferior to the rib cage. Place a 5 mm trocar high up in the median epigastrium.
Start your free 3-day trial — no credit card required, full access included
Position the camera trocar in the left upper quadrant, ensuring it is at least 15 cm away from the xiphoid.
Insert another two 12 mm trocars in the median epigastrium inferior to the rib cage. Place a 5 mm trocar high up in the median epigastrium.
Skeletonize the greater curvature of stomach by transecting the gastrocolic ligament close to the gastric wall, while preserving the gastroepiploic arteries. Start the distad dissection with the Ultracision at the inferior gastric body, ending 3-5 cm proximal of the pylorus. Open the lesser sac and take down any adhesions to the pancreas.
Activation of this course for 3 days.
Most popular offer
Combine our learning modules flexibly and save up to 50%.
US$86.85/ yearly payment
Unlock all courses in this module.
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.
Activation of this course for 3 days.
Most popular offer
Combine our learning modules flexibly and save up to 50%.
US$86.85/ yearly payment
Unlock all courses in this module.
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.