
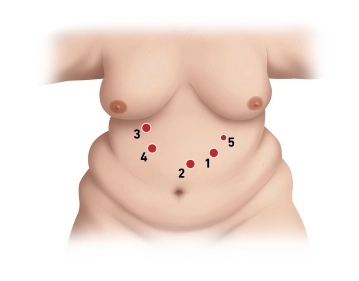
The position of the camera trocar is in the left upper abdomen, approximately 2-3 fingerbreadths below the left costal margin in the midclavicular line.
Access is achieved using an optical trocar (12mm Xcel trocar) under camera view. During insertion, visualization of the individual tissue layers is ensured. Further trocar placement is performed under camera view and after positioning in the anti-Trendelenburg position.
Three additional 12mm trocars are then placed in the following order. First, approximately 1.5 handbreadths below the xiphoid process paramedian left (far supraumbilical), then approximately in the midclavicular line immediately at the right costal margin, with the trocar tip directed towards the patient's left lower extremity. The third 12mm trocar is finally inserted approximately one handbreadth below the right costal margin medial to the midclavicular line in the right upper abdomen, and lastly, an additional 5mm trocar at the left costal margin slightly cranial to the first 12mm trocar.
Note: A liver retractor is used only in extremely large livers, which is the case in less than 5% of patients.