
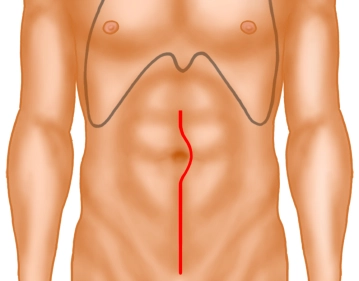
Median laparotomy, starting at the symphysis up to a few centimeters above the umbilicus. (It is very important to ensure that the skin incision is actually carried down to the symphysis, as otherwise access to the pelvis is significantly impeded). If necessary, some mobilization of the bladder. Insertion of a drape (foil) and a retractor. Intraoperative assessment of findings.
-
Skin incision and exposure
![Skin incision and exposure]()
Soundsettings -
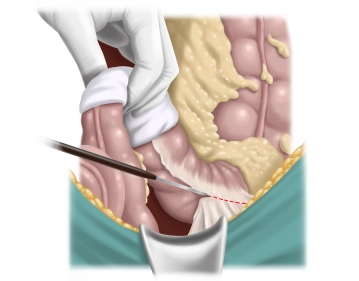
Mobilization of the left flexure
![Mobilization of the left flexure]()
Soundsettings The mobilization of the left flexure is performed alternately from aboral by dissecting the descending colon in an avascular plane in front of the left kidney and from oral by detaching the greater omentum from the colon up to approximately the middle of the transverse colon with opening of the omental bursa. Finally, the connections to the spleen and pancreas are released.
-
Lateral mobilization of the sigmoid
![Lateral mobilization of the sigmoid]()
Soundsettings The colon is retracted medially and the lateral adhesions with the peritoneum lateral to the abdominal wall are sharply divided. Care must be taken to ensure that the dissection is not carried too deeply, that is, down to the psoas and behind the kidney, but rather only the mesosigmoid is mobilized. The ureter will then automatically come to lie dorsally and can be identified. Exposure in the sense of a ureterolysis is not required.
-
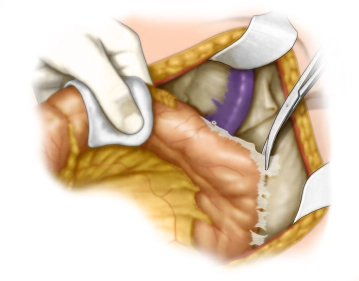
Division of the inferior mesenteric vein
![Division of the inferior mesenteric vein]()
Soundsettings Opening of the mesocolon from centrally below the duodeno-jejunal junction (ligament of Treitz). In doing so, the inferior mesenteric vein can be exposed near the lower border of the pancreas and divided between Overholt clamps.

Division of the inferior mesenteric artery
Now, the inferior mesenteric artery is sought by first incising the peritoneum at the base of the m
Now, the inferior mesenteric artery is sought by first incising the peritoneum at the base of the m
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.23 / module
US$86.85/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.47
/ month
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.