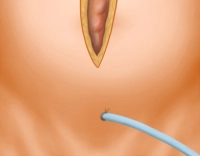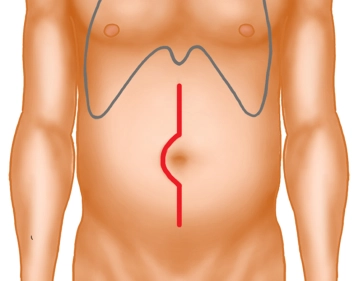
Median midline laparotomy with right-sided umbilical incision. Transection of subcutaneous fat tissue and fascia with monopolar diathermy.
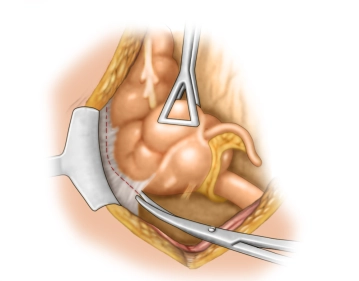
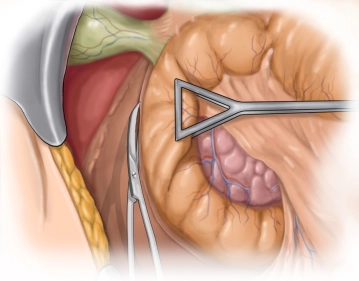
After transection of the peritoneum, insertion of a suprapubic bladder catheter. Positioning of the surgical site with the retractor system.