
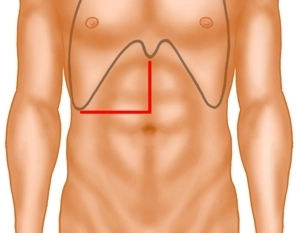
The laparotomy begins with a right-sided transverse incision at the level of the navel and is then extended in the midline supraumbilically to the xiphoid. Examination of the abdominal organs to exclude further metastases, confirmation of resectability.
-
Laparotomy; Exploration
![Laparotomy; Exploration]()
Soundsettings -
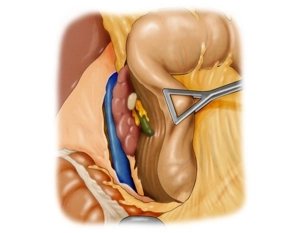
Mobilization of the Duodenum according to Kocher
![Mobilization of the Duodenum according to Kocher]()
Soundsettings The liver is elevated and the duodenum is mobilized and retracted medially to such an extent that the inferior vena cava is accessible in its full length.
Note: Detachment of the right colonic flexure may additionally be necessary depending on the operating field (not required in this example).
-
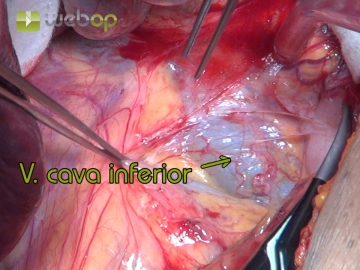
Depiction of the Right Retroperitoneum with Cranial and Medial Displacement of the Liver
![Depiction of the Right Retroperitoneum with Cranial and Medial Displacement of the Liver]()
Soundsettings To achieve a sufficiently good depiction of the right adrenal gland, which is retroperitoneal and located directly under the liver next to the inferior vena cava, it is necessary to displace the liver cranially and medially. First, the parietal peritoneum covering the front of the lower part of the adrenal gland is opened parallel to the inferior vena cava.
Note: Surgical procedures on the right retroperitoneum are more challenging than on the left side, as liver enlargement, obesity, or a barrel chest can significantly complicate the positioning of the surgical site.
Mobilization of the liver from caudal; preparation at the inferior vena cava
Next, the adhesions between the liver surface and the adrenal gland are severed. Due to the peritum
Next, the adhesions between the liver surface and the adrenal gland are severed. Due to the peritum
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.
TachoSil<sup>®</sup> Versiegelungsmatrix
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.