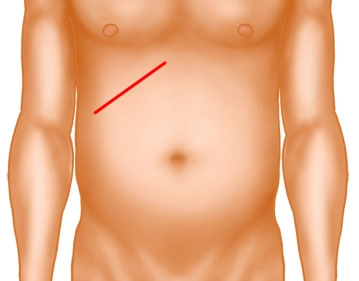
The preferred access route is the transverse upper abdominal laparotomy on the right. This incision can be extended to the left as desired. Before laparoscopic surgery could become established, the right subcostal incision (Kocher) (see image above) was traditionally recommended.
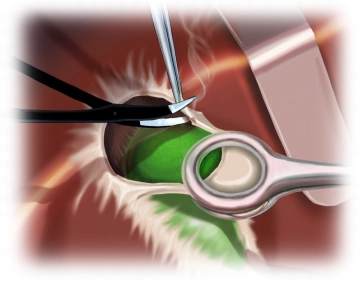
After cutting through the skin, the subcutaneous fatty tissue is sharply divided up to the anterior leaf of the rectus sheath. Then the fascia is opened and the rectus abdominis is transversely divided with diathermy. By using a Kocher retractor, which is bluntly pushed under the muscle, thermal injuries to dorsal structures can be avoided. In the lateral part of the incision, the M. obliquus externus, internus, and M. transversus abdominis are divided. The then exposed posterior rectus sheath / transversalis fascia is carefully opened together with the peritoneum, sparing intra-abdominal structures.
Note:
Pararectal incisions are obsolete.
The length of the incision always depends on the individual circumstances.
Never cut directly at the costal margin, as in this case not enough tissue is available for wound closure.
In case of an enlarged liver, the incision can also be made significantly more caudal.