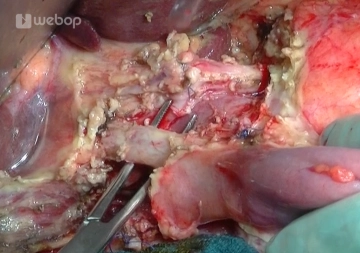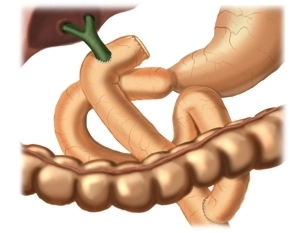
The end-to-side hepaticojejunostomy with a retrocolically routed upper jejunal loop excluded from the passage by Roux-Y anastomosis represents the gold standard of biliodigestive anastomosis.
In this case, the biliodigestive anastomosis is preferably created above the cystic duct insertion and approx. 2–3 cm below the hepatic bifurcation.
- The widest possible anastomosis opening should be created (if the bile duct is too narrow, widening procedures are recommended, e.g. after Hepp-Couinaud).
- The suture with single-row full-thickness interrupted sutures should be primarily watertight.
- Precise adaptation of the bile duct mucosa to the intestinal mucosa must be ensured.