
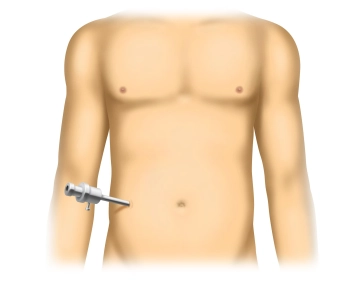
After sterile washing and draping of the entire abdomen from the costal margin to the symphysis, an open entry into the abdomen is made through a small incision placed contralateral to the hernia. Blunt insertion of a 10 mm trocar, establishment of pneumoperitoneum, the intra-abdominal pressure should be approximately 12-15 mmHg.
-
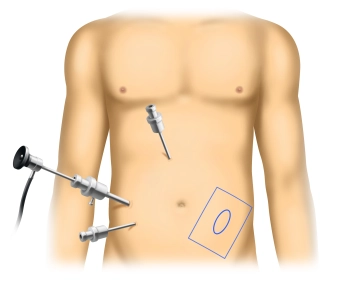
Positioning, skin incision, pneumoperitoneum
![Positioning, skin incision, pneumoperitoneum]()
-
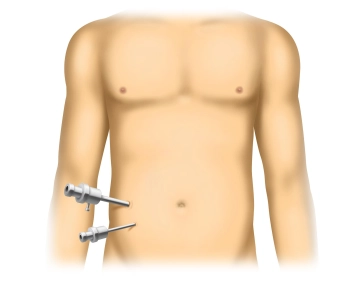
Insertion of the optics and working trocars
![Insertion of the optics and working trocars]()
Introduce the camera optics and inspect for possible injuries or bleeding: Particular attention should be paid to adhesions in the immediate vicinity of the first trocar. After an orienting laparoscopy, introduce a 5mm working trocar. This is always done under vision and is therefore relatively safe. The exact location must be determined by the surgeon based on their preferences and experience. A second working trocar will be positioned later.
-
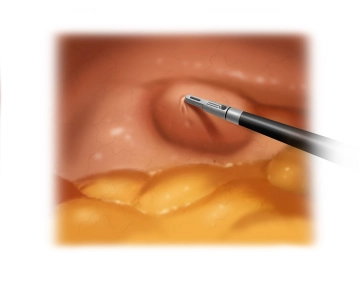
Inspection of the hernia orifice
![Inspection of the hernia orifice]()
Inspection of the hernia orifice. This typically penetrates the fascia of the transversus abdominis muscle and the internal oblique muscle in the area of the linea semilunaris (curved line marking the transition of the rectus abdominis muscle into the adjacent tendon plate), while the superficially located fascia of the external oblique muscle usually remains intact. The predilection site of Spiegel's hernia is the intersection between the linea semilunaris and the linea arcuata.
-
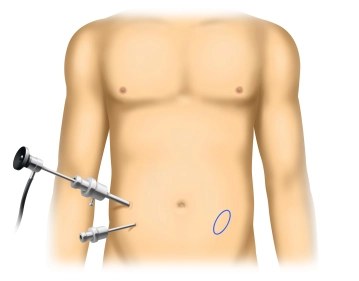
Determine the size and location of the hernia defect
![Determine the size and location of the hernia defect]()
Marking the center of the hernia gap and determining the hernia boundaries with a percutaneously inserted needle and recording on the skin. To determine the required mesh size, the exact location of the hernia center must be known.
Note: If there is an incarceration of the hernia contents, which may consist of mesh or bowel, this incarceration must first be subtly released.
-
Selection of the optimal network size
![Selection of the optimal network size]()
Positioning of a second 5mm working trocar under direct vision. Once the hernia is precisely marked on the skin, the size of the mesh can be determined. The mesh should extend at least 5 cm beyond the outer edge of the hernia defect on all sides. Drawing the mesh and the entry points for the holding sutures. This ensures that the pre-placed sutures are later brought out at exactly the right spot, allowing the mesh to be optimally centered over the hernia defect.
Positioning of the mesh
Placement of a total of 4 holding sutures using monofilament thread at four points of the mesh. The
Placement of a total of 4 holding sutures using monofilament thread at four points of the mesh. The
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
€7.99 inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from €3.70 / module
€44.50 / yearly payment
general and visceral surgery
Unlock all courses in this module.
€12.42
/ month
€149.00 / yearly payment