
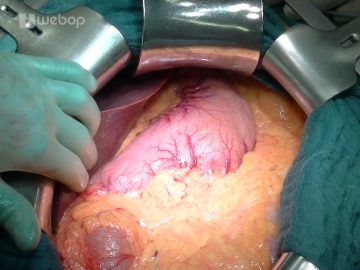
Opening of the abdomen via a transverse upper abdominal laparotomy approx. 3-4 fingerbreadths below the costal arch with transection of cutis, subcutis, anterior fascial sheath, M. rectus abdominis and posterior fascial sheath/peritoneum. The ligamentum teres hepatis is transected between clamps and secured with transfixion ligatures (Vicryl® 2-0). The falciform ligament is released using monopolar current extending high above the liver. After covering the abdominal walls with moist abdominal towels, the frame retractor system consisting of an abdominal wall frame and a cable pull retractor system such as the Ulm retractor is inserted. Subsequently, systematic exploration of the abdominal cavity is performed: Liver (metastases?), Stomach (tumor?, position of the nasogastric tube), Small intestine (adhesions?, peritoneal carcinomatosis?), Colonic frame (tumor?), Greater omentum (adhesions?, peritoneal carcinomatosis?).
-
Transverse Upper Abdominal Laparotomy
![Transverse Upper Abdominal Laparotomy]()
Soundsettings -
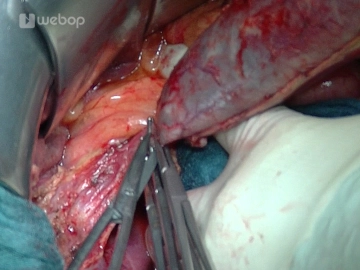
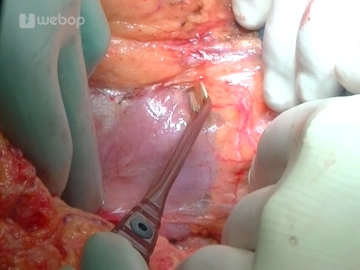
Antegrade Cholecystectomy
![Antegrade Cholecystectomy]()
Soundsettings The resection phase begins with the cholecystectomy: Grasping of the gallbladder and antegrade mobilization from the liver bed using bipolar forceps and scissors, exposure of the cystic duct and cystic artery, which are each grasped with an Overholt clamp, then transected and secured with a transfixion ligation (Prolene® 3-0). After detachment and removal of the gallbladder, a swab is taken from the bile secretion.
-
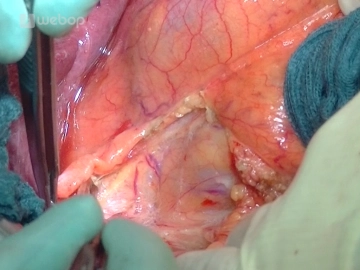
Mobilization of the right colonic flexure/Kocher maneuver
![Mobilization of the right colonic flexure/Kocher maneuver]()
Soundsettings To mobilize the right colonic flexure, the peritoneal fold lateral to the ascending colon is incised, and the incision is continued around the right flexure. By gentle traction on the colon, the avascular connective tissue layer dorsal to the colon is tensed, and the mesocolon can be detached from the retroperitoneal space, from the anterior surface of the duodenum and the pancreatic head.
The mobilization of the duodenum is performed according to Kocher: the mobilized colon segment is shifted to the left side, and the duodenum, after incision along its outer edge using bipolar forceps and dissecting scissors, is released together with the pancreatic head from its retroperitoneal connections. The mobilization of the pancreatic head is continued over the aortic plane up to the ligament of Treitz, so that the pancreatic head can be completely encircled or palpated from the dorsal side (tumor size? consistency?).
-
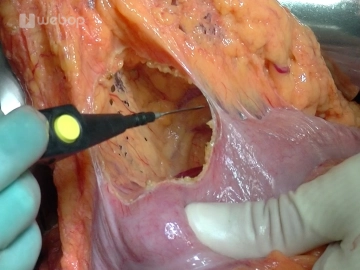
Opening of the Bursa omentalis
![Opening of the Bursa omentalis]()
Soundsettings Entering the Bursa omentalis by detaching the omentum from the right colic flexure to the left third of the transverse colon. The Bursa omentalis is slightly adhered, but can be well freed and exposed with the bipolar forceps. Now the pancreas can also be well explored on the left side.
-
Exposure of the Inferior Pancreatic Border and the Mesentericoportal Venous Axis
![Exposure of the Inferior Pancreatic Border and the Mesentericoportal Venous Axis]()
Soundsettings Continue the preparation at the inferior pancreatic border with exposure of the superior mesenteric vein and the portal vein. In doing so, the veins of the pancreatic head are divided using LigaSure® or between transfixion ligatures (Prolene® 4-0 or 5-0). The pancreas can now be tunneled starting from caudal at the level of the superior mesenteric vein/portal vein and provided with stay sutures on its inferior border left and right of the portal vein.
Caution: Bleeding from the portal vein! -as little traction on the tissue as possible!
After opening the lesser omentum and exposing the common hepatic artery at the upper border of the
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
US$86.85/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.