
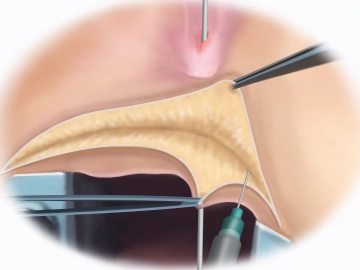
The procedure begins with the insertion of the anal speculum and the probing of the rectovaginal fistula, which in the film example appears as a connection between the rectum and the lower third of the vaginal canal. To facilitate dissection, physiological NaCl solution is initially injected percutaneously using the so-called infiltration technique. Then, the slightly curved access over the perineum is made using an electrosurgical needle. After transecting the subcutaneous tissue, the anal retractor is inserted.
-
Fistula Probing, NaCl Injection, and Transverse Incision at the Perineum
![Fistula Probing, NaCl Injection, and Transverse Incision at the Perineum]()
Soundsettings -
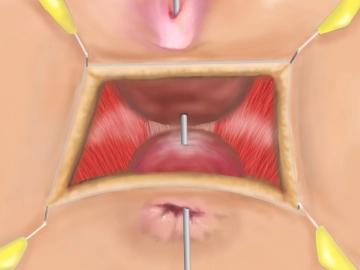
Preparation of the Rectovaginal Space; Display of the External Sphincter and Puborectalis Muscle
![Preparation of the Rectovaginal Space; Display of the External Sphincter and Puborectalis Muscle]()
Soundsettings Dissection of the rectovaginal space using an electronic needle with subtle hemostasis. The preparation must extend beyond the fistula tract and allow for the secure identification of the levators lateral to the vagina and anorectum. The goal is to approximate the levator muscles as a barrier between the posterior vaginal wall and the anterior rectal wall as described in the following steps.
Preparation of the Sphincter Stumps
To prepare for sphincter reconstruction, the muscle stumps are located. The preparation is facilita
To prepare for sphincter reconstruction, the muscle stumps are located. The preparation is facilita
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.