Functionally, the rectum represents a fecal reservoir that prevents continuous fecal discharge. It connects directly to the sigmoid colon and, similar to it, exhibits an S-shaped a/p and lateral curvature (flexura sacralis, anorectalis, and lateralis). Typically, the rectum is divided into three sections:
1. Ampulla recti (main reservoir, ventral to the sacrum)
2. Anal canal (see below, closure region between the anorectal flexure and the skin opening)
3. Between 1 and 2, an unspecified section that emerges at a right angle from 1 and similarly transitions at a right angle into 2. Here, typical folds are found in the mucosa (Kohlrausch folds).
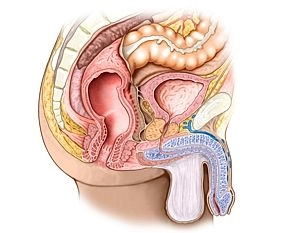
Adjacent structures of the rectum are dorsally the sacrum and coccyx, laterally next to the internal iliac A. and V. the regional lymph nodes, the sacral plexus and parts of the autonomic nervous system as well as ureters and adnexa. Ventrally, in the female organism, uterus and vagina, in the male the urinary bladder and prostate/seminal vesicles. Caudally is the pelvic floor.