
In rectal prolapse, the rectum protrudes through a lax pelvic floor musculature and strong straining facilitated by the anus to the outside. In rare cases, the protruded bowel can become trapped and require emergency surgery. With prolonged prolapse, the sphincter muscle can be so damaged that stool can no longer be retained (fecal incontinence).
The initial therapy involves avoiding straining through stool regulation. However, in most cases, surgery is necessary. Depending on age and the extent of symptoms, abdominal and perineal/transanal surgical procedures can be applied.
-
Rectal Prolapse
![Rectal Prolapse]()
-
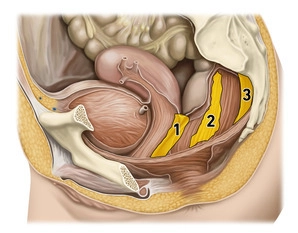
Pelvic Floor
![Pelvic Floor]()
(1) Rectogenital septum, (2) Paraproctium, (3) Mesorectal fascia
The pelvic floor forms the muscular closure of the caudal abdominal cavity as a "functional unit" and prevents the prolapse of the intestines or pelvic organs. The pelvic floor structures support the intestinal and urogenital closure system, with the muscular components playing a crucial role in support and continence function. Muscular overstretching or denervation can lead to pelvic floor descent (descent) or to various forms of organ prolapse in the small pelvis. Women are far more frequently affected than men (gender ratio 9:1).
The development of pelvic floor insufficiency is generally a multifactorial process. The most common causes of pelvic floor disorders include the number of vaginal deliveries, excessive straining during defecation, obesity, and previous surgical interventions in the small pelvis.
-
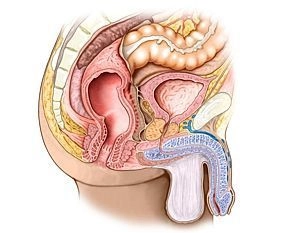
Rectum
![Rectum]()
Functionally, the rectum serves as a fecal reservoir that prevents continuous defecation. It directly follows the sigmoid colon and, similar to it, exhibits an S-shaped anterior-posterior and lateral curvature (sacral, anorectal, and lateral flexures). Typically, the rectum is divided into three sections:
1. Ampulla recti (main reservoir, ventral to the sacrum)
2. Anal canal (see below, closure region between the anorectal flexure and the skin opening)
3. Between 1 and 2, there is an unspecified section that emerges at a right angle from 1 and transitions at a right angle into 2. Here, typical folds (Kohlrausch folds) are found in the mucosa.
Adjacent structures of the rectum include, dorsally, the sacrum and coccyx, laterally alongside the internal iliac artery and vein, the regional lymph nodes, the sacral plexus, and parts of the autonomic nervous system, as well as the ureter and adnexa. Ventrally, in females, the uterus and vagina are located, while in males, the bladder and prostate/seminal vesicle are present. Caudally, the pelvic floor is situated.
Anal Canal
1) Longitudinal muscular layer, (2) Circular muscular layer, (3) Levator ani muscle, (4) Puborectal
1) Longitudinal muscular layer, (2) Circular muscular layer, (3) Levator ani muscle, (4) Puborectal
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.