
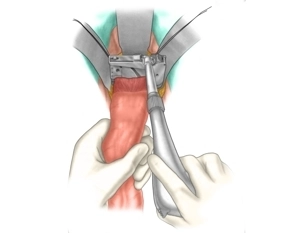
The technique is demonstrated using a descendorectostomy (see also open rectal resection) . The rectum is transected using a linear stapling device.
-
Transection of the Rectum
![Transection of the Rectum]()
Soundsettings -
Preparation of the intestinal wall of the descending colon
Soundsettings The intestinal section to be anastomosed is freed from adherent tissue over a distance of 5-10 mm.
Placement of a purse-string suture on the proximal stump
First, the proximal bowel stump is cleaned and disinfected with a swab (e.g., with Betadine) (not s
First, the proximal bowel stump is cleaned and disinfected with a swab (e.g., with Betadine) (not s
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.20
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.14 / module
US$85.75/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.29
/ month
US$171.50 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.