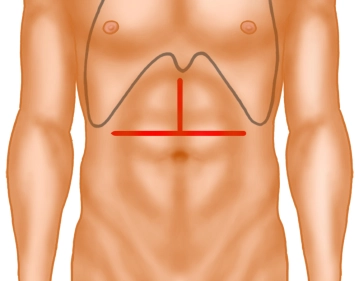
Open the abdomen via a transverse upper abdominal incision with upper midline extension, the so-called "inverted T".
Transect the subcutaneous tissue with electrocautery, tunnel both rectus muscles with a nonmetal probe and divide them with electrocautery.
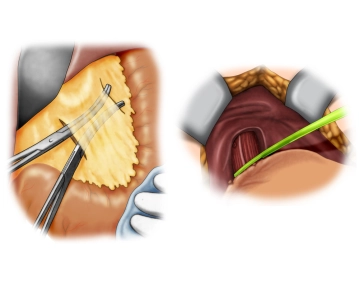
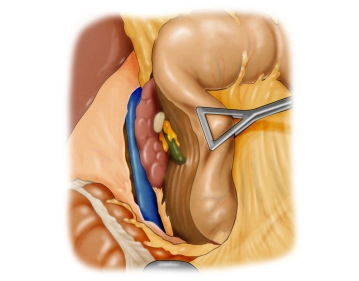
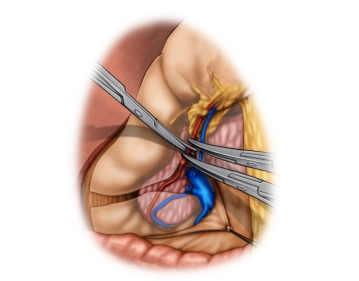
Explore the abdominal cavity to assess the location and extent of the tumor and thus its resectability after ruling out distant metastases, specifically in the peritoneum and liver. In this case the tumor is in the middle third of the stomach at the large curvature.