
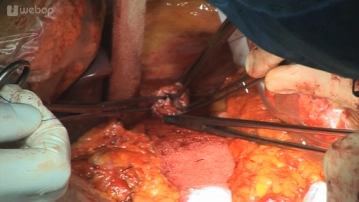
Open the distal esophagus by transverse transection of its anterior wall and secure it proximally with an Allis forceps; this will prevent the distal esophagus from retracting craniad into the mediastinum. Now transect the posterior wall of the esophagus. Preplace a purse string suture (monofilament, nonabsorbable, 2/0, continuous full-thickness over-and-over) and gently dilate the esophagus with a dressing forceps. Insert the anvil of a circular EEA stapler and secure it by tying the preplaced purse string suture.
-
Anchoring the anvil with a purse string suture
![Anchoring the anvil with a purse string suture]()
Soundsettings -
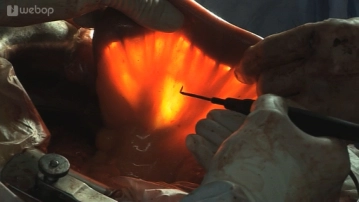
Assessing the jejunal arcades and determining the length of the afferent limb
![Assessing the jejunal arcades and determining the length of the afferent limb]()
Soundsettings In order to achieve a good functional result, the segment of the jejunum must be dissected sufficiently long. To this end, lift the transverse colon craniad, hold up and spread the jejunal mesentery and under transillumination with the surgical light assess the arterial supply of the second jejunal loop. The intestine and mesentery of the efferent limb should be transected such that the transected end of the limb will easily reach the esophagus.
-
Dissecting the Roux limb
-
Retrocolic transposition of the Roux limb into the upper abdomen


Esophagojejunal anastomosis
Fashion the anastomosis with the esophagus in end-to-side technique with the circular EEA stapler b
Fashion the anastomosis with the esophagus in end-to-side technique with the circular EEA stapler b
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.40
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.29 / module
US$87.56/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.59
/ month
US$175.10 / yearly payment