
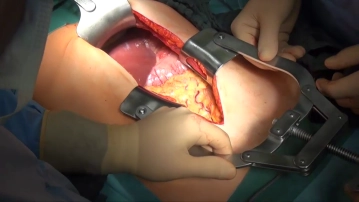
Opening of the abdomen through an upper midline incision, which is extended caudally with a left-sided circumcision of the navel. After the insertion of abdominal retractors and spreaders, exploration of the abdominal cavity is performed with assessment of the location and extent of the primary tumor, lymph node involvement, and organ metastases.
-
Access
![Access]()
Soundsettings -
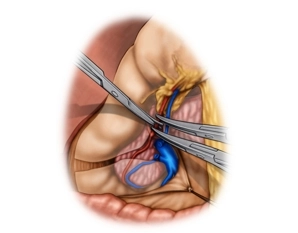
Detachment of the Greater Omentum; Resection of the Gastroepiploic Vessels
![Detachment of the Greater Omentum; Resection of the Gastroepiploic Vessels]()
Soundsettings The greater omentum is lifted and tensioned against the transverse colon with controlled traction. The greater omentum is dissected directly at the upper edge of the transverse colon, and the omental bursa is opened.
After mobilization of the right colonic flexure and the descending part of the duodenum, as well as careful separation of the greater omentum adhered to the mesocolon on the right side, the resection of the gastroepiploic vessels entering here is performed. The right gastroepiploic vein is transected before its confluence into the superior mesenteric vein, and the corresponding artery is severed at its origin from the gastroduodenal artery. -
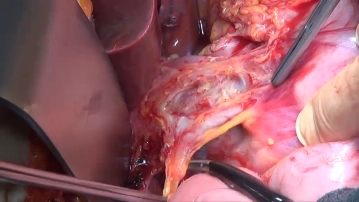
Lymphadenectomy I (Lig. hepatoduodenale/Station 12 and 13)
![Lymphadenectomy I (Lig. hepatoduodenale/Station 12 and 13)]()
Soundsettings The lymphadenectomy (LAD) begins at the hepatic hilum, includes the Lig. hepatoduodenale, and continues along the common hepatic artery to the celiac trunk.
After performing the cholecystectomy, which is not detailed here, the liver-proximal incision of the lesser omentum is made with bipolar scissors, starting left-laterally of the Lig. hepatoduodenale and continuing up to the level of the cardia. Lifting the connective tissue along with the lymph nodes (LN) contained within it over the common hepatic artery at the left edge of the Lig. hepatoduodenale using forceps and exposing the artery. Gradual detachment of the LN tissue bundle (Station 12) over the portal vein and the common bile duct. By inserting the index finger into the Foramen of Winslow, the common and proper hepatic arteries, portal vein, and possibly suspicious lymph nodes can be palpated with the thumb and index finger. Then clearing out LN Station 13 between the pancreatic head and the inferior vena cava.
-
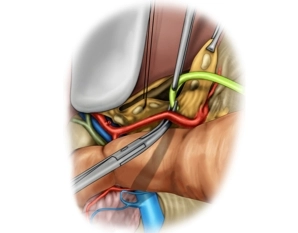
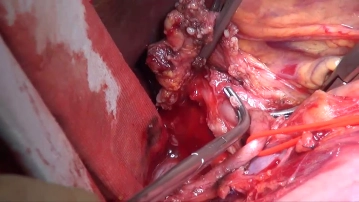
Lymphadenectomy II (Common Hepatic Artery/Station 8)
![Lymphadenectomy II (Common Hepatic Artery/Station 8)]()
Soundsettings The right gastric artery is transected and ligated between Overholt clamps. After looping the proper hepatic artery, the lymph node tissue bundle (Station 8) is pulled craniomedially and gradually dissected completely using bipolar scissors along the common hepatic artery towards the celiac trunk, ensuring that the dissection occurs directly at the adventitia of the vessels, as the lymph nodes are adjacent to them. Looping the common hepatic artery with a vessel loop simplifies the preparation. The dorsal boundary of the lymph node dissection is the anterior surface of the inferior vena cava.
-
Lymphadenectomy III (Celiac Trunk/Station 9)
![Lymphadenectomy III (Celiac Trunk/Station 9)]()
Soundsettings The origins of the common hepatic artery and the splenic artery from the celiac trunk are exposed as previously described and freed from the lymph node tissue bundle. With the proximal transection of the left gastric artery and the removal of the lymph node tissue bundle, the lymphadenectomy is complete. The origin of the celiac trunk and the aorta are not dissected free.
Resection of the Stomach
Using an organ grasping forceps applied to the greater curvature, the stomach is gently pulled cran
Using an organ grasping forceps applied to the greater curvature, the stomach is gently pulled cran
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.23 / module
US$86.85/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.47
/ month
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.
TachoSil<sup>®</sup> Versiegelungsmatrix
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.23 / module
US$86.85/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.47
/ month
US$173.70 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.