Position the patient head down and on the right side, then exploration and confirmation that the sigmoid tumor is not visible. Next, display the vascular axis of the inferior mesenteric artery and vein and inspect the pelvis. A dilative angiopathy with significant kinking of the pelvic vessels is observed.
In the right hemiabdomen, multiple adhesions to the anterior abdominal wall are evident. Initially, a careful adhesiolysis is performed following appendectomy and transverse upper abdominal laparotomy for cholecystectomy (not shown).
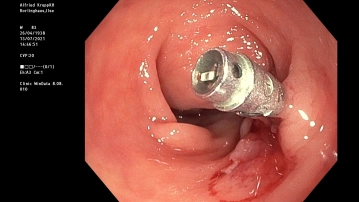
Now, an intraoperative colonoscopy is performed to locate the tumor. For this, the sigmoid-descending junction is clamped with a soft grasping forceps. The endoscopy shows the finding in the middle of the sigmoid. The tumor area is marked endoluminally with a clip.
Note: In cases where tumors are not macroscopically visible, intraoperative endoscopic marking is a sensible measure.