
Excision of the old upper abdominal right-angle laparotomy following previous atypical metastasis resection in the area of the posterior right liver segments. Preparation down to the peritoneum and opening of the abdomen.
-
Access
![Access]()
Soundsettings -
Adhesiolysis
Soundsettings Significant adhesions are encountered in the upper abdomen, making exploration of the abdomen to exclude an extrahepatic tumor and peritoneal carcinomatosis initially only partially possible. Both the right colonic flexure and small bowel loops are adherent to the liver and must be sharply dissected step by step. Then, reposition the wound edges and insert the retractor.
-
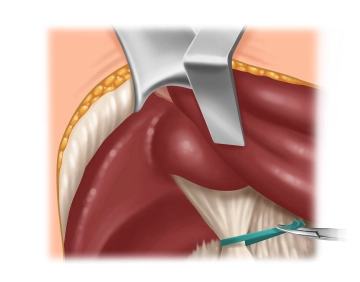
Liver Hilum Preparation
![Liver Hilum Preparation]()
Soundsettings Next, the hepatoduodenal ligament is dissected out of the scar tissue and looped with a Mersilene band. This allows for temporary hilum occlusion (Pringle maneuver) in case of intraoperative bleeding complications.
A lymph node dissection is not performed, as it was already done during the primary procedure, and no enlarged lymph nodes are observed upon inspection and palpation.
Note:
In principle, lymph node dissection of the liver hilum is recommended for colorectal liver metastases, as the incidence, depending on the number and location of the metastases, is reported to be 3-28%.
Mobilization of the Liver
To achieve adequate exposure of the posterior segments, the liver must be completely freed from the
To achieve adequate exposure of the posterior segments, the liver must be completely freed from the
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.20
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.14 / module
US$85.75/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.29
/ month
US$171.50 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.