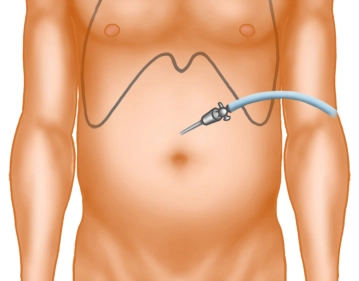
A small skin incision is made well above the navel in the midline. After inserting the Veress needle and verifying the correct position, the pneumoperitoneum is established.
-
Skin incision
![Skin incision]()
Soundsettings -
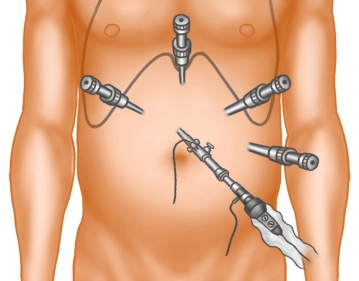
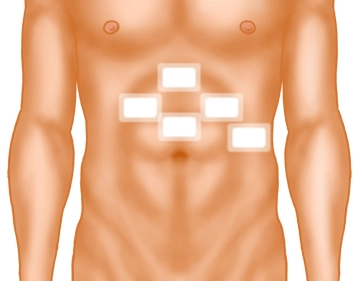
Trocar positioning
![Trocar positioning]()
Soundsettings The optics are introduced via a 5mm/10mm trocar. A diagnostic laparoscopy is performed. Under direct vision, 4 trocars are placed in the upper abdomen.
-
Traction of the stomach and incision of the lesser omentum
![Traction of the stomach and incision of the lesser omentum]()
Soundsettings The left liver lobe is held up with the laparoscopic probe and the stomach is tensed with the Babcock clamp. In the area of the pars flaccida, the lesser omentum is incised with the ultrasonic scalpel.
-
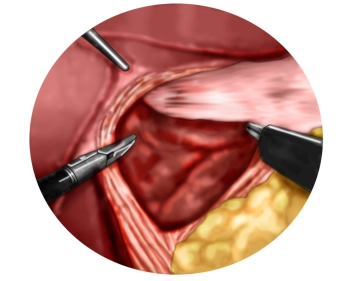
Preparation of the diaphragmatic crura with entry into the mediastinum
![Preparation of the diaphragmatic crura with entry into the mediastinum]()
Soundsettings Now the right diaphragmatic crus is displayed. Then, proceed anteriorly over the anterior commissure to the left diaphragmatic crus and display it as well. In doing so, the ventral mediastinum is opened.
-
Preparation of the lower esophagus
![Preparation of the lower esophagus]()
Soundsettings One now proceeds far into the lower mediastinum and circumferentially mobilizes the lower esophagus from its adhesions. In doing so, the posterior vagus nerve is clearly identified and remains with the esophageal musculature. The esophagus is mobilized from the mediastinum to the extent that the area of the lower esophageal sphincter is tension-free in the abdominal cavity.
-
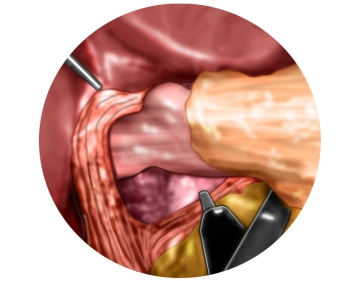
Mobilization of the gastric fundus
![Mobilization of the gastric fundus]()
Soundsettings The gastrosplenic ligament and the short gastric vessels are transected at the level of the splenic hilum along the greater curvature up to the upper pole of the spleen and further to the left diaphragmatic crus until the gastric fundus is completely mobilized.
-
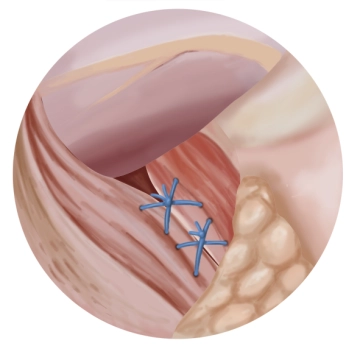
Posterior hiatoplasty
![Posterior hiatoplasty]()
Soundsettings A posterior hiatoplasty is performed using two Z-sutures (braided, non-absorbable suture size 1). The passage for the esophagus must remain sufficiently wide and well patent.
Tip: To avoid constriction of the terminal esophagus by the hiatoplasty, it is recommended to introduce a gastric tube Charrière (Ch) 40 as a calibration bougie transorally.
-
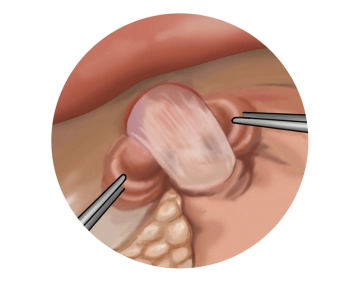
Shoeshinetest
![Shoeshinetest]()
Soundsettings The fundus portion located near the His angle is pulled to the right side. The corresponding fundus portions are now located using the shoeshine test.
-
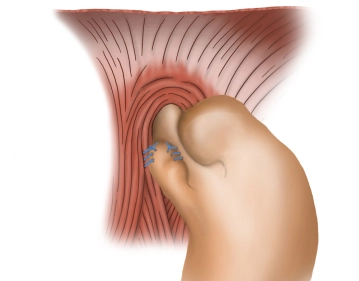
Fixation of the fundus cuff I
![Fixation of the fundus cuff I]()
Soundsettings The anterior vagus branch is clearly identified. While preserving it, the right fundus flap is initially continuously sutured to the right side of the esophagus (braided, non-absorbable suture size 2-0). Additionally, the fixation of the fundus portion pulled to the right is then performed with another continuous suture (braided, non-absorbable suture size 2-0) to the right diaphragmatic crus.
-
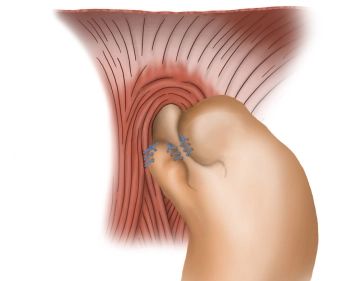
Fixation of the fundus cuff II
![Fixation of the fundus cuff II]()
Soundsettings In the manner of a Toupet fundoplication (270°, open at the front), the corresponding left-sided portion of the fundus is attached to the left side of the esophagus with an additional suture (braided, non-absorbable thread size 2-0).
-
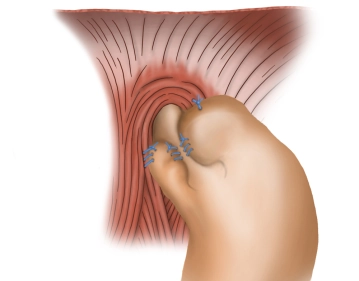
Fixation linker fundus
![Fixation linker fundus]()
Soundsettings With another suture, the left fundus portion is fixed to the diaphragm (braided, non-absorbable suture size 2-0).
-
Suture and Dressing
![Suture and Dressing]()
Soundsettings After confirming hemostasis, instruments and trocars are withdrawn under direct visualization. Layered closure of the working ports is performed with sutures and dressing.