
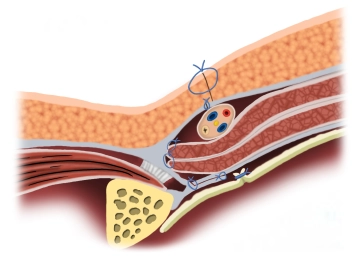
Duplication of the transversalis fascia and attachment of the transversus muscle and internal oblique muscle to the inguinal ligament for reconstruction and stabilization of the posterior wall of the inguinal canal.
-
Principle
![Principle]()
-
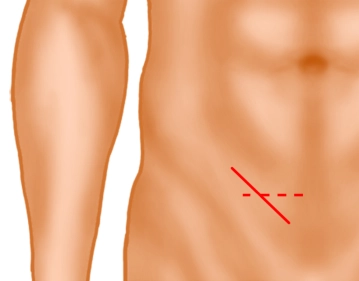
Inguinal skin incision
![Inguinal skin incision]()
Soundsettings A skin incision approximately 5 cm long is made obliquely two fingerbreadths above the inguinal ligament (solid line) or alternatively a transverse skin incision two fingerbreadths above the pubic bone. Subsequently, the subcutaneous tissue is incised down to the external oblique aponeurosis. Subcutaneously located superficial epigastric vessels are ligated (not shown).
-
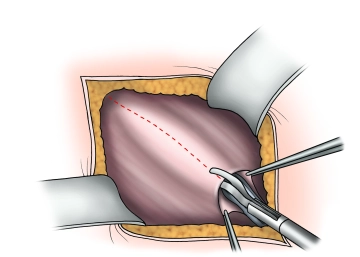
Splitting of the external aponeurosis
![Splitting of the external aponeurosis]()
Soundsettings The external aponeurosis is opened parallel to the fibers, including the external inguinal ring, extending beyond the level of the internal inguinal ring. The fascial edges are clamped, elevated, and the fascia is bluntly separated from the internal oblique muscle and the cremaster muscle.
Attention: The iliohypogastric nerve lies on the internal oblique muscle!
Identification of the hernial sac; looping of the spermatic cord
The transversalis fascia is exposed up to the symphysis. After looping the spermatic cord at the le
The transversalis fascia is exposed up to the symphysis. After looping the spermatic cord at the le
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.