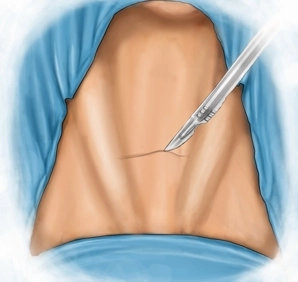
It is made caudal to the thyroid cartilage and approximately 1-2 fingerbreadths above the jugular fossa as a roughly 3 cm long transverse skin incision. Then, division of the subcutis and platysma to the superficial cervical fascia.
-
The Skin Incision
![The Skin Incision]()
Soundsettings -
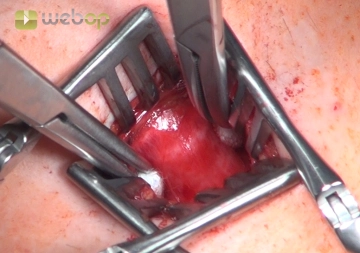
Access to the Trachea
![Access to the Trachea]()
Soundsettings After transverse transection of the superficial cervical fascia, a median incision of the pretracheal lamina and dissection into the depth. With two wound retractors, the ventral tracheal wall in the area of the third and fourth tracheal rings is optimally positioned, with the straight neck muscles being spread apart; if necessary, the thyroid isthmus must be pulled cranially.
Note: If the thyroid isthmus does not release the anterior tracheal wall, it is resected and the resection margin is sutured around both thyroid lobes.
-
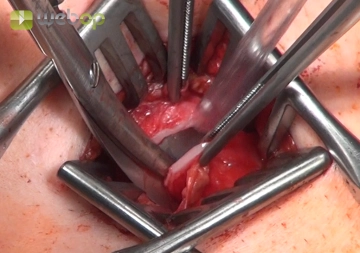
The Opening of the Tracheal Window
![The Opening of the Tracheal Window]()
Soundsettings The opening of the trachea is preferably performed between the second and third tracheal cartilage rings. The intercartilaginous ligament (Lig. anulare) is incised across the entire width of the anterior tracheal wall with a scalpel. Subsequently, the third and fourth cartilage rings along with the intervening Ligamentum anulare are cut on both sides of the lateral tracheal wall using scissors. This creates a window flap incision with a caudal base.
Note: When incising the trachea, it is important to ensure that the cuff of the trans-laryngeally placed tube is not within the surgical field. If necessary, deeper intubation should be performed to avoid damaging the cuff. Only in this way can the procedure be completed with good visibility.
-
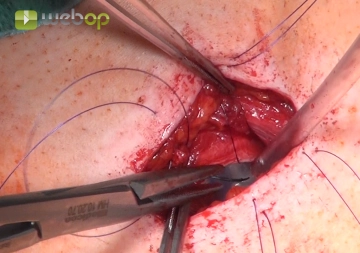
The Transcutaneous Fixation of the Window Flap
![The Transcutaneous Fixation of the Window Flap]()
Soundsettings After careful hemostasis, the epithelialization of the tracheostomy is performed by adapting the skin to the edge of the tracheal opening. First, the "window flap" is sutured with the skin in the caudal wound area, then the mobilized upper skin edge is fixed to the trachea, each with individual button sutures (slowly absorbable monofilament 4-0) using a backstitch technique.
-
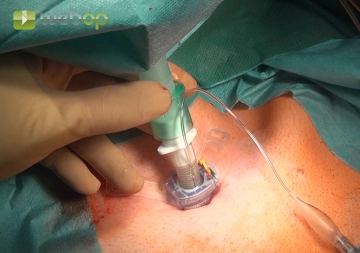
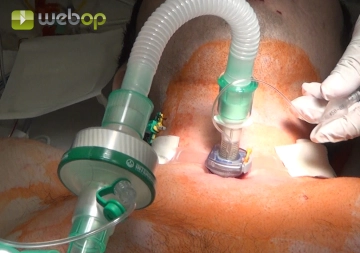
The Introduction and Connection of the Tracheostomy Tube
![The Introduction and Connection of the Tracheostomy Tube]()
Soundsettings Under visualization, the translaryngeal tube is deflated and withdrawn by the anesthesiologist. After suctioning the tracheal secretions, a size 9 tracheostomy tube is introduced through the tracheostoma. Once the cuff is inflated, the tube is connected to the ventilator.
-
The External Fixation
![The External Fixation]()
Soundsettings After verifying proper ventilation, the tracheostomy tube is secured around the patient's neck with a holding band.