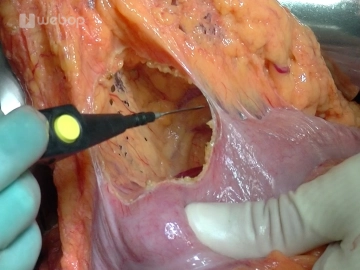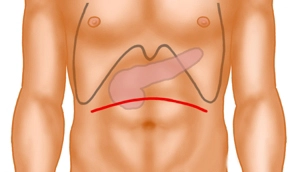
The approach is a curved, cranially convex, transverse upper abdominal laparotomy. Subsequently, the exploration phase involves inspection and palpation of the entire abdomen to exclude distant metastases and signs of local unresectability.
After inserting a sheet as abdominal wall protection, a pulley hook system is used.
Note:
Alternatively, in cases of a very acute costal angle, a median laparotomy may be performed.