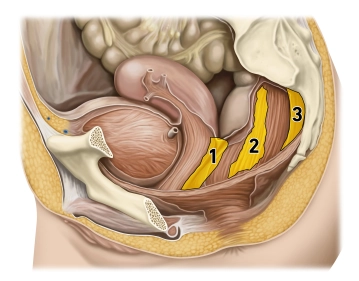
(1) Rectogenital septum, (2) Paraproctium, (3) Mesorectal fascia
The pelvic floor forms the muscular closure of the caudal abdominal cavity as a "functional unit" and prevents the prolapse of the intestines or pelvic organs. The pelvic floor structures support the intestinal and urogenital closure system, with the muscular components playing a crucial role in support and continence function. Muscular overstretching or denervation can lead to pelvic floor descent (descent) or to various forms of organ prolapse in the small pelvis. Women are much more frequently affected than men (gender ratio 9:1).
The development of pelvic floor insufficiency is generally a multifactorial process. The most common causes of pelvic floor disorders include the number of vaginal deliveries, excessive straining during defecation, obesity, and previous surgical interventions in the small pelvis.