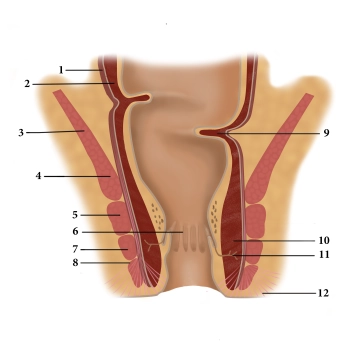
(1) Tunica muscularis longitudinale, (2) Tunica muscularis circulare , (3) M. levator ani, (4) M. puborectalis, (5) M. sphincter ani profundus, (6) Columnae anales, (7) M. sphincter ani superficialis, (8) M. sphincter ani subcutaneus, (9) Kohlrausch fold, (10) M. sphinkter internus , (11) Proctodeal gland, (12) M. corrugator ani
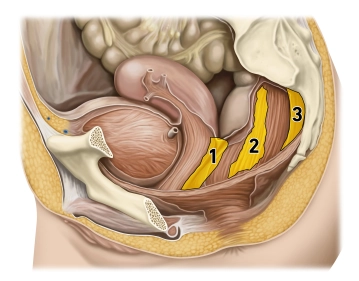
Three muscles form the closure apparatus in the wall of the lower rectum:
1. The M. sphincter ani internus represents a thickening of the last circularly running fibers of the smooth colon muscle and is innervated by the sympathetic nervous system.
2. The M. levator ani, on the other hand, is voluntarily innervated (Plexus sacralis) and the M. puborectalis attached to the pubic bone is also attributed to it. It pulls as a large loop around the anal canal ventrally and thereby functionally kinks it.
3. The M. sphincter ani externus is also striated and suspended between the center of the perineal region (Centrum perinei) and the coccyx. It is voluntarily innervated by the N. pudendus. Through its contraction, the anal canal is terminally closed. The different innervation of the three closing muscles provides additional security against failures and resulting incontinence.
In the mucosa of the anal canal, there are numerous longitudinally running folds (Columnae anales), which exhibit dense arterial (!) plexuses with venous drainage. Upon contraction of the sphincter muscles, they fill up quickly and the mucosa swells, lies against each other, and thus forms a gas-tight closure. Hemorrhoids and venous thromboses are well-known vascular complications of this region.
Defecation occurs on the one hand through the relaxation of the closure mechanisms (initiated by the voluntary musculature, emptying of the erectile tissues) and on the other hand through active abdominal press and the peristalsis of the intestine.