

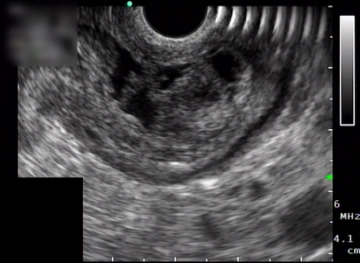
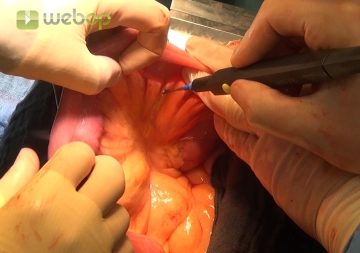
The endoscopic examination reveals a submucosal tumor of the gastric wall obstructing the gastric outlet.

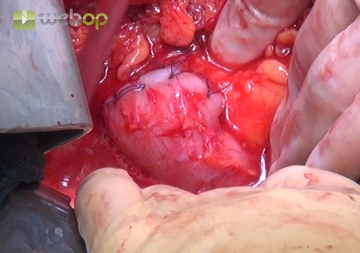



Active local hemostasis and sealing
TachoSil® Versiegelungsmatrix
TachoSil® is used in adults and children from 1 month of age as supportive treatment in surgery for improving hemostasis, for supporting tissue sealing, and for suture support in vascular surgery when standard techniques are insufficient. TachoSil® is used in adults for supportive sealing of the dura mater to prevent postoperative cerebrospinal fluid leakage after neurosurgical procedures.
Produktwebsite TachoSil®
TachoSil® Prescribing Information 05-2025 (354.1 kB)