The main problem in flexor tendon surgery is the tendency for adhesions and scarring between the tendon and the flexor tendon sheath. The only feasible way to avoid such adhesions so far is through early movement of the tendon.
For this, a stable suture technique is needed that must meet high requirements.
Thread guides in which the thread encircles the tendon fibers in such a way that tightening the suture results in the loop closing (locking suture) are significantly stronger (10–50 %). A classic method of this type is the Kirchmayr-Kessler suture shown here (Fig. 1), in which the threads are appropriately backstitched during loop formation.

The tensile strength of this two-strand suture is sufficient to withstand the stress of passive aftercare. It is technically simple and therefore well applicable in practice. However, a two-strand suture is not sufficient to withstand the stress of active aftercare without resistance. For surgical success, a dynamic Kleinert aftercare is therefore mandatory, which requires a sufficient degree of patient cooperation in the first weeks postoperatively.
This is repeatedly a critical point, therefore in recent decades new suture techniques have been proposed (Fig. 2) that allow higher loads.
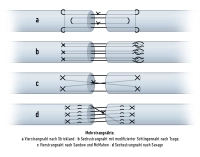
These are technically more demanding and not without complications. The classic Kirchmayr-Kessler suture therefore remains the method of first choice for many hand surgeons for the reconstruction of a severed flexor tendon.
The case shown here involves a 9-day-old laceration at the ulnopalmar aspect of the right ring finger middle joint in a young patient.