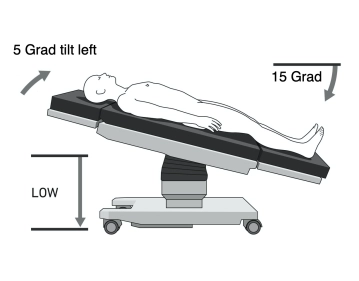
- Patient placed in supine position on a vacuum cushion; left arm optionally abducted
- Operating table adjusted to 15° anti-Trendelenburg and tilted 5° left
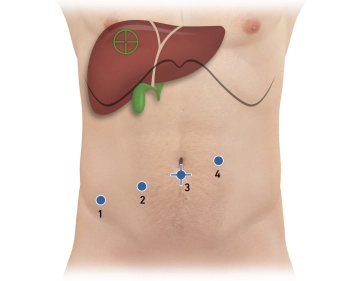
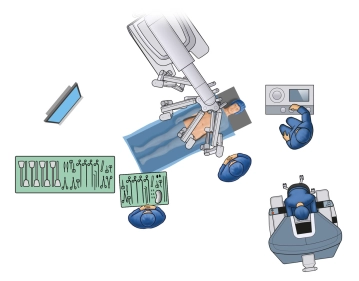
- Robotic arms docked from the right or cranial-right position
Important Notes:
- Docking alignment is critical; without a table-motion function, undocking is required for table adjustments. Ensure vacuum cushion integrity before draping
Assistants and nursing staff position themselves to the patient’s left, while anesthesia is stationed at the head
The robot (Patient Cart) is positioned from the right or right cranial side and docked. The surgeon operates from the console, ideally with a view of the patient.