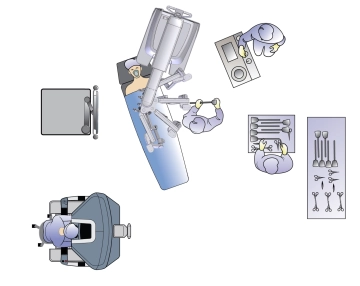
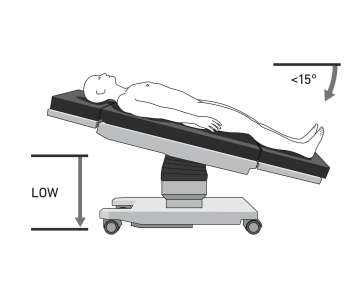
The patient is positioned in a supine position on the large vacuum cushion. The left arm can be positioned away from the body. The use of the cushion eliminates the need for any additional supports. The table assistant sits to the left of the patient. The video tower is positioned on the right at torso height. Anesthesia is located at the head of the patient, and the surgical nurse is to the left of the table assistant. The patient is placed in a 15-degree reverse Trendelenburg position before docking.
Caution: Positioning is of particular importance due to the docking of the patient to the robot's manipulator. There is a risk of injury to the abdominal wall if the patient slips.
Note: Vacuum cushions may have leaks. Check again before sterile draping.