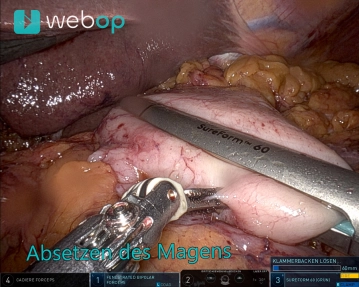
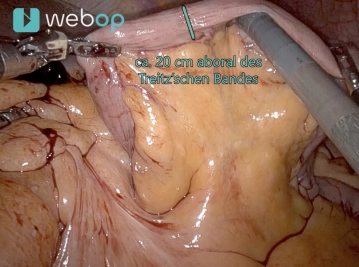
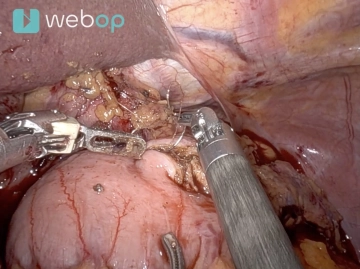
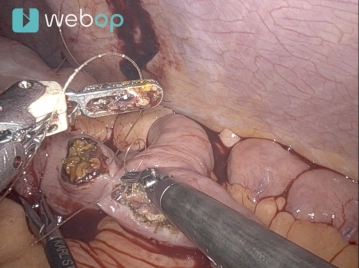
Now work with two right arms for stapling (stapler on the 12 mm trocar, third from the right from the patient's perspective). The duodenum is circumferentially exposed 2-3 cm aboral to the pylorus. The duodenum is then transected with a robotic stapler (Sure Form 60 mm, blue cartridge).
Caution: Before transecting the duodenum, the gastric tube should be fully withdrawn or at least safely removed from the stomach.
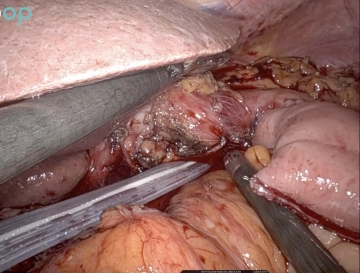
Switch back to the configuration with two left hands. Now the stomach is placed in the left upper abdomen and the liver is lifted ventrally with the Cadiere. Completion of the lymphadenectomy along the common hepatic artery from the trunk to the origin of the gastroduodenal artery. When the crossing left gastric vein appears, the vessel is clipped centrally twice, peripherally once, and transected.
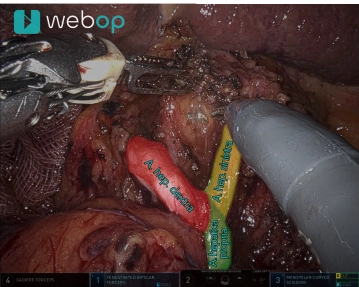
Then lymphadenectomy is performed along the splenic artery starting at the celiac trunk until the origin of the left gastroepiploic vessels is reached. These vessels remain intact to ensure the blood supply to the remaining stomach. Regardless, lymphadenectomy can be performed up to the splenic hilum. Finally, the origin of the left gastric artery at the trunk is identified, and the vessel is clipped centrally twice and peripherally once with purple Hemoloc® clips and transected.
Caution: During lymphadenectomy, the pancreatic capsule should remain intact. Otherwise, very troublesome pancreatic fistulas with behavioral situations at the upper edge of the pancreas can occur.
Note: The management of the left gastric artery is safest and clearest when both the common hepatic artery and the splenic artery are already cleanly dissected.