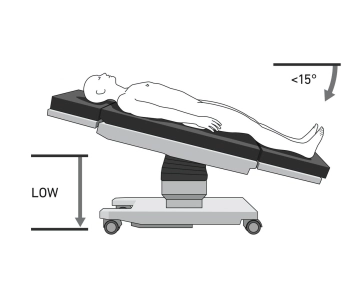
The patient is positioned in a supine position with a slight reverse Trendelenburg position of approximately 10-15 degrees on the large vacuum cushion. The left arm is positioned on an arm support rail to the side to keep the surgical area clear and to optimize access for the surgical team and the robotic arms. The use of the vacuum cushion typically eliminates the need for additional supports, which speeds up preparation.
Note: The precise positioning of the patient is crucial for the success of the surgery, as it ensures optimal access of the robotic arms to the surgical sites in the abdominal cavity and minimizes the risk of complications.
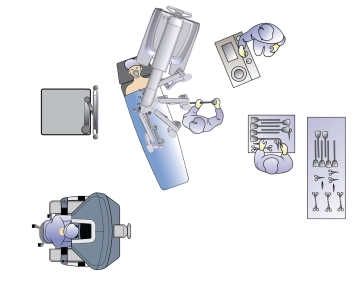
The surgical team usually consists of two surgeons: the console surgeon, who controls the robot from a console, and the table assistant, who assists directly at the operating table. The table assistant is seated to the left of the patient. The video tower, which transmits the images from the robotic camera, is positioned on the right at torso height. Anesthesia is located at the head of the patient. The OR nurse stands to the left of the table assistant.
Caution: Correct positioning is of particular importance due to the docking of the patient to the robot's manipulator. Incorrect positioning or slipping of the patient during the operation poses a significant risk of injury to the abdominal wall by the robotic arms or instruments. Therefore, a careful check of the positioning before the start of the operation is essential.
Remark: Vacuum cushions can develop leaks over time. Before the sterile draping of the patient, the integrity of the vacuum cushion must be checked again to ensure a secure and stable hold of the patient throughout the procedure. Regular maintenance of the vacuum cushions is also advisable.