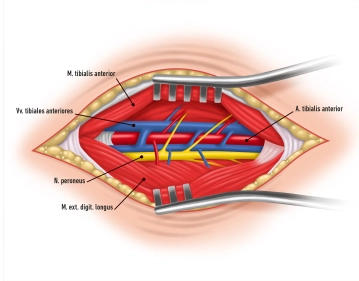
The skin incision is made with slight internal rotation of the leg approximately two fingerbreadths lateral to the anterior edge of the tibia. Hemostasis. Incision of the anterior fascia initially with a scalpel, then with half-open dissecting scissors. The tibialis anterior muscle and extensor digitorum longus muscle are bluntly separated.
Tips:
1. The length of the skin incision must be adapted to the depth of the surgical area. Since the crural skin-soft tissue mantle is very vulnerable, surgery should under no circumstances be performed under skin tension, which must also be observed during instrumental wound retraction.
2. To avoid injuries to the peroneal nerve, the skin incision should not be made too close to the fibular head.
3. The exposure of the lower leg arteries must be as atraumatic as possible. The use of magnifying glasses is recommended.
4. Due to the arteriosclerotic remodeling of the vessel wall, a local inflammatory concomitant reaction is not uncommon, which can be particularly pronounced in diabetics (note the soft tissue edema in the film clip!). The preparation of such vessel segments can quickly become unclear due to the occurrence of diffuse bleeding.